






Infant co-sleeping is a fraught topic. On social media, in particular, co-sleeping (sharing a bed with your baby) and sleep training exist on two sides of a spectrum. Both are praised by some and vilified by others, and there is little compromise or nuance to be had. One difference, though, is that it’s easy to find medical experts (pediatricians, in particular) who support sleep training. Pediatricians who advocate for infant co-sleeping are fewer, especially given the American Academy of Pediatrics guidelines on it (more on those below).
The broad medical strictures against co-sleeping have pushed this behavior into the shadows. The problem with that is it leaves parents without the data on risks to make their own best decisions.
This article is about infant co-sleeping, especially in the first six months of life, when the risk of SIDS is the highest. Once a child is older, bigger, and able to kick you in the face (for example), the co-sleeping risks are extremely small. You may or may not choose to co-sleep with an 18-month-old, but that is a choice about what works for you and your family sleep-wise.

How common is infant co-sleeping?
Our best data on infant co-sleeping prevalence in the U.S. comes from a set of surveys called the Pregnancy Risk Assessment Monitoring System, or PRAMS, which are run at the state level and ask new parents a series of questions about their baby. These surveys are done early in life, with an average age of around 4 months and virtually all infants under 6 months — in other words, the ideal age group to evaluate the prevalence of infant co-sleeping.
In the 2016 PRAMS data, 55% of women surveyed said they “always” had their baby sleep in a separate sleeping area, and 18.7% said they did so “often.” This means that 45% of families are co-sleeping at least some of the time with an infant, and about a quarter are doing so most of the time. These figures may underestimate the actual prevalence, given possible concerns about revealing this information to a surveyor.
Co-sleeping in these data is more common for women with less education and less income, although these differences are fairly small.
The share of families who reported putting their babies on their back to sleep is much higher — around 80% — suggesting that some of the standard advice about sleep is being followed more closely than others.
Why do some people choose to co-sleep?
Many people find bed-sharing to be convenient and use it as a way to get more sleep — if you try to move an infant who has fallen asleep, they tend to wake up. If the baby wakes up less, parents may sleep more.
Another common reason people tend to co-sleep is the possibility of improved success with breastfeeding. Certainly, there is a correlation: moms who bed share are more likely to be breastfeeding. But this doesn’t necessarily point to causality. We know from data that women who have a strong desire to breastfeed before they give birth are more likely to bed share. It could be that the desire to breastfeed prompts bed sharing, not the other way around. And indeed, there is little data to support links between bed sharing and breastfeeding success.
This doesn’t necessarily mean there are no benefits for your family to bed sharing, just that it probably isn’t a panacea to improve your breastfeeding success.
What does the data say about safety?
The core worry about co-sleeping is that it may increase the risk of SIDS. Infants who are sleeping with an adult are at risk of the adult rolling onto them, or at risk from the blankets and pillows in the bed. One study that did a careful analysis of sudden infant deaths found that, of those that could be explained, about 75% were a result of soft bedding and 20% a result of adult overlay. Many remained unexplained, however, and this result does not directly speak to the magnitude of the risk of co-sleeping.
There is no ethical way to do a randomized trial on this topic. In lieu of that, the best option would be to recruit a very large number of families, collect data on sleep behavior (and other variables), and follow them over time. The dataset would need to be extremely large because, thankfully, SIDS risk is very small. In order to have statistical power to distinguish risks across groups, you would need a lot of data. This type of study does not exist.
The data we do have comes from case-control studies. In this type of study, researchers begin with a sample of “cases,” in this case, babies who died from SIDS, and they identify a set of “controls” — babies who are otherwise similar (in age, demographics, etc.) but did not die. They survey families about their sleep behavior, among other things. These studies have many problems (notably, issues with parental recall), but they are sometimes the only way to study rare outcomes.
A 2013 meta-analysis does, in my view, the best job of combining the studies on bed sharing to produce some estimates of the risks. The paper attempts to identify the risk of bed sharing with and without the presence of other risk factors. The graph below shows the absolute SIDS risk (deaths per 1,000 live births) for different behavior patterns. (Note that in this paper, breastfeeding appears slightly predictive against SIDS, which doesn’t hold up in the best versions of the data.)
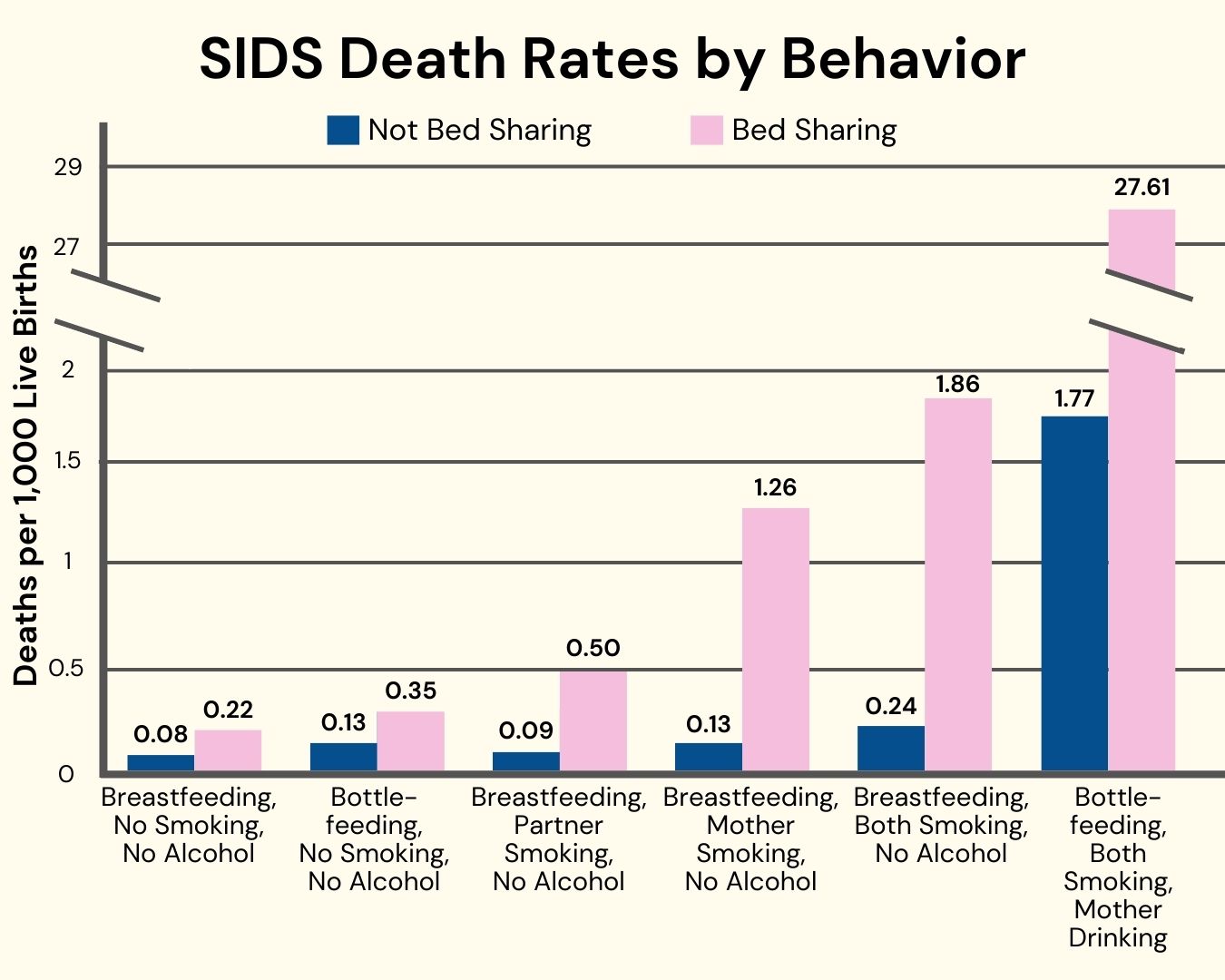
From this, I would highlight a few key takeaways.
- Even in the safest configuration (no adults smoking or drinking), researchers still estimate a slightly increased risk of SIDS with bed sharing.
- However, this increased risk is very small, about 0.15 per 1,000 births. It’s hard to think about small numbers with such a terrifying event, but to put it in context, the overall infant mortality rate in the U.S. is about 5 in 1,000.
- Most importantly, the risks of bed sharing are very small relative to other risk factors, notably smoking. SIDS risk is higher when parents smoke, even if they do not bed share. The risks with smoking, alcohol use, and bed sharing are significantly elevated.
This analysis makes clear that within the category of bed sharing, risks vary widely depending on what else you are doing. A related point: co-sleeping on a sofa or in an armchair is much higher-risk than in a bed. This is important to say in part because parents will sometimes end up in an armchair with their baby because they are trying to stay awake and not co-sleep. It would be far safer to purposely co-sleep in a flat-surface bed, without blankets and pillows, than to fall asleep accidentally in the chair.
The upshot here seems to be: co-sleeping does carry some small risks, but these risks vary greatly by the circumstances of co-sleeping. If people are going to co-sleep, there are definitely safer and less safe ways to do that.
What is the medical guidance people are given?
The data bottom line suggests the value in a nuanced set of advice. In an ideal world, parents would be given a full rundown of the data and then some guidance on how to choose for themselves.
This isn’t the way the advice is constructed. In its latest guidelines, the AAP states, “…on the basis of the evidence, the AAP is unable to recommend bed sharing under any circumstances.” The evidence the authors cite is the study referenced above. Helpfully, they do go on to discuss the circumstances that make bed sharing more and less safe. But the headline point has limited nuance.
Perhaps because of this, the data suggest that in many cases, parents are not getting advice about this from their providers. The same PRAMS data that shows us the prevalence of co-sleeping also asked parents about sleep advice. Almost 93% of parents said they got advice about putting their baby to sleep on their back; only 48% heard from their provider about not bed sharing.
It’s not clear why the direct AAP advice is not being given in the same way for bed sharing as it is for back sleeping, but I would guess it is partially about provider hesitance to give advice they know may be ignored. This is a missed opportunity — better communication could literally save lives.
Closing thoughts
Is co-sleeping right for you? I have no idea! This is an area where many decisions seem like reasonable ones, based on a combination of personal preference, constraints, and resources. What we can say confidently from the data is that if you are going to co-sleep, make sure your baby is put to sleep on their back, that you limit blankets and pillows in the bed, and that you do not smoke. And never co-sleep on the sofa.
The bottom line
- Despite the AAP strongly discouraging it, about 45% of U.S. families co-sleep with their infants at least some of the time for a variety of reasons, including improving sleep and perceived breastfeeding success (although the data does not support this claim).
- Co-sleeping does slightly increase SIDS risk, but the absolute risk is very small. If you do choose to co-sleep, there are safer (and less safe) ways of doing so.
- The risks with smoking, alcohol use, and bed sharing are significantly elevated.
- If you are going to co-sleep, make sure your baby is put to sleep on their back, that you limit blankets and pillows in the bed, and that you do not smoke or drink alcohol. And never co-sleep on the sofa.












Log in
What about sharing a room with a parent as they get older? My husband and 4 year old sleep on same room. This works for us logistically. Any downside?
I’d like to know how the research that shows a higher risk of SIDS in the context of cosleeping defines cosleeping. The article appears to imply that the 0.22 per 1,000 figure would be lower if dangerous cosleeping was categorised as different from safer environments like a flat mattress. Is that correct? Would love an answer to this!
It seems from what is written that the risks of co-sleeping are more related to suffocation than SIDS? (As to me it seems that if a death is explained by suffocation it’s not SIDS?) but would be curious on the science/classification there, perhaps that is incorrect.
What about bassinets that attach to the bed, like this one? https://www.petiteamelie.be/co-sleeper-nuage-walnoot.html?utm_source=google-surfaces&utm_medium=organic&gad_source=1&gad_campaignid=23123498310&gbraid=0AAAAACnXFtsQ8d8nSxwvqOt_n9tPYJEqT&gclid=Cj0KCQiAiebIBhDmARIsAE8PGNJ0cwEP8Xj3IX4Yd91OR8d5s-6WZ-wzbZGtwrgaBCfkJvkpx9Ez4dsaAiHhEALw_wcB
Is this as safe as a stand-alone bassinet? Would any of the elevated risks of co-sleeping also apply to this arrangement? For example, if my partner smokes, would the risk be higher with an attached bassinet as opposed to a standalone one? Thanks
My understanding is that the cosleeper you posted is great, as long as the bedding is flat and the child bed is empty without pillows, blankets, or toys. I don’t know about the smoking, but though that had more to do with the smoke inhalation itself vs. behavior of smokers. Maybe it’s both?
I believe that when something is both natural and deeply intuitive for a mother and baby, that instinct matters. When co-sleeping is approached intentionally and safely, many parents experience meaningful benefits that are not reflected here. The article does not acknowledge the importance of bonding for the baby’s emotional regulation, nor the role close contact can play in supporting maternal emotional stability and strengthening the mother-baby bond. This is not simply about getting more sleep or making breastfeeding easier. For many families, it is about biology, instinct, emotional security, and connection.
Modern science often seeks measurable proof, yet not everything that shapes early development can be easily captured in data. Maternal attunement, instinct, and the biological drive for proximity are powerful forces. Across cultures and throughout history, babies have slept near their caregivers, and that is not inherently unsafe when done with intention and knowledge of safe sleep practices.
SIDS is a serious concern, and unsafe environments like couches and soft bedding clearly increase risk. That must always be taken seriously. At the same time, there is room for nuance. When co-sleeping is done safely, some families experience benefits that matter, including stronger bonding, improved responsiveness, and a deepened sense of connection and security for both mother and baby.
Reducing this discussion to only risk and data overlooks the very real emotional and biological foundations of early attachment. Instead of discouraging maternal intuition, we should support a balanced approach that respects safety and honours the natural instinct for closeness that many mothers and babies share.
Why isn’t alcohol mentioned in your closing thoughts? If I am reading the graph correctly alcohol seems to be the cause of the vast majority of SIDS cases, not bed sharing.
And marijuana. Drugs of any type should not be used by anyone who shares a bed, not just by the mother.
Just made this update. Thank you!
There are cultural dimensions to this. This was 20 years ago now, but one of my friends was hosting a West African college student at their house (he was Ghanaian or Nigerian can’t remember which) and she had just had her first baby. He was horrified to hear to that she put her baby to sleep in a crib and called it child abuse and neglect. He said every mother from his community always had their baby in their bed, that whenever the baby woke up, it would just nurse from the mother and the mother usually slept through the night. He thought it was so strange that westerners would subject themselves to waking up all the time and force their babies to be away from them.
Also, in Korea and Taiwan my friends have stuffed in their babies cribs all the time and have told me that they weren’t told it was a sids risk. So guidelines aren’t universal.
even knowing the overall risk is low … I’ve never understood why parents are willing to assume additional risk. I had twins who each slept in a bedside bassinet. Yes it was hard, yes they woke up all the time, especially in the first 5-6 months before sleep training, but they never ended up in our bed. I slept so much better knowing they were in a safe sleep space within arm’s reach, while I could sleep exactly as I liked – foam mattress topper, heavy duvet, etc. It was worth it to me to get even an hour of quality sleep at a time and get up to feed them rather than have them in the bed.
Fast forward to them now – they’re two years old and still happy as clams in their crib where they sleep peacefully all night long.
Is there data about this with exclusively breastfed babies who are exclusively bottlefed?
In the TLDR, it mentions that the data does not show improvement in breast feeding or attachment but this is not mentioned in the body of the article. What does is the data on this?
I wish I had known all of this earlier in my parenting journey. I was determined to be a safe sleeper for the first 6 months- then I was gifted a precious bundle of joy who DID NOT SLEEP unless held. So we took turns holding him on the couch- which I now know is SO MUCH MORE DANGEROUS. My Ped never recommended co-sleeping but was clear that couch / lounger was so much more dangerous than bed when we went in desperate to figure out why he would not sleep (spoiler alert- it’s because he was a baby and biological need to be close is normal). Later down the road when I did end up cosleeping some, I learned the Safe Sleep 7, my partner left the bed, we removed all except my pillow, and my blanket. We are now 18 months and still end up in bed every night, I still make my partner leave the bed, we have rails etc. It just makes me sick to think about how little we knew and how uneducated we were at first and how much unknowing risk we took.
at 18 months your partner sleeps outside the bed every single night? Have you considered the impacts on them of this setup?
shes saying what works for her and sharing her experience. There’s no need to attempt to shame under the guise of asking a question. We don’t need to be like that here or anywhere else. Let’s assume she’s a thoughtful person and able to consider the same things in her family that we are able to consider in our own families and let her be.
We never intentionally co-slept but sometimes we wound up in a haze of exhaustion with the baby in the bed for a while. I struggle to understand how an adult could sleep without pillows and blankets. Sleeping on a hard surface without a pillow sounds awful and unworkable to me. I don’t disagree with the recommendations here, but I can’t imagine how I would have adhered to them.
Full-time cosleeper here, and this probably depends on your sleep habits, but for me… it’s just not that hard to use a pillow and blanket and keep them off of my baby’s face. I have so much awareness of my baby in the bed, even when I’m asleep. Maybe some people fling their pillows around in their sleep? I don’t; it’s under my own head. And these precautions are focused on babies who aren’t mobile yet, so it’s not like they’re going to crawl under the blanket on their own. I have to wonder how often this advice is actually followed, and how many of the people who successfully co-sleep are doing it in a relatively normal bed setup and possibly afraid to admit they do.
I do have a firm mattress, and it visibly makes sense that a baby who can roll onto their stomach would not be safe on a plush mattress topper where their little face is going to sink way in.
I slept on the edge of the pillow with the majority of the pillow behind me away from baby, and blankets never went higher than my waist (Kyte baby also makes adult sleep sacks for very cold nights). Never did my child ever end up in a safe position (he’s a healthy 2.5 year old now). The hard mattress was not fun, though.
The smoking, soft bedding, and adult overlay risks remind me of how important the Safe Sleep Seven are for parents who choose to co-sleep:
1. No smoking
2. Sober parents
3. Breastfed (mixed data on this, as noted above)
4. Unswaddled baby, lightly dressed
5. Baby is full-term and healthy
6. Placed to sleep on back
7. On a safe surface. This most likely means a very firm mattress, on the ground, devoid of pillows, blankets, stuffed animals, other children, and pets. Parents should also make sure there are no strangle risks, like phone chargers, that come onto the bed.
Since so many parents end up co-sleeping, intentionally or accidentally, it would be good to see more education around doing it as safely as possible.