






My oldest child is a teenager now, and when I think back on the first days with her, there are moments that stand out brightly — like when our friends brought pastries to the hospital — but much of it is a blur. I know a lot of it was hard, but it’s distant enough now that I forget quite how hard.
But when I look back at notes I, or my husband, took at the time, I can see clearly just how hard and isolating that early period was. I know this experience is not unusual or unique. Every week on social media or in email, I hear from people asking, basically, “I’m drowning. Does this get better?”
It’s not only the first weeks — postpartum mental health can be a roller coaster for many months. Even if the first weeks seem easy, later months can get tough.
As I put it in Cribsheet, “Before the baby, you’re a vessel to be cherished and protected. After the baby, you’re a lactation-oriented baby accessory.” The physical realities post-childbirth are often jarring, even if you are prepared, and so are the mental hurdles. You may understand in the abstract that emotional ups and downs are common, but that’s different than living through them.
This post focuses on the data on mental health — what we know about postpartum mental health issues and what helps. Let me start with the most important point: if this resonates with you, if you’re suffering, please get help. Your OB can help, and a perinatal psychiatrist or other therapist is a great resource. One place to start if you can’t access any of these is Postpartum Support International.

Beyond the “baby blues”
Let’s start with the basics: although we do not discuss it enough, postpartum depression, postpartum anxiety, and even postpartum psychosis are common. The primary reason for this is hormonal. In the first days and weeks after your baby arrives, there are rapid hormonal shifts. Estrogen and progesterone drop, the hormones responsible for breastmilk increase, and generally, things are in flux. This hormonal storm impacts almost everyone.
Most women find they are emotionally sensitive during this period. I spent our first visit with friends crying in a spare bedroom for an hour for no reason (they didn’t bat an eye, gave me a hug, and brought me food on a tray. Lesson: only visit friends like this).
This early experience is sometimes referred to as the “baby blues” and is self-limiting in the sense that the hormone surge is worst in the first couple of days after giving birth and has died down by a couple of weeks later.
But true postpartum depression or other postpartum mental health conditions can crop up in this period. They can also arise later, even months later. Many women discount later-onset depression, thinking postpartum depression only happens right after the baby arrives. This is not the case.
The prevalence of postpartum depression, even if we focus only on diagnosed cases, is high. An estimated 10% to 15% of women who give birth will experience it. The data suggest that about half of these women actually experience the onset of depression during pregnancy; post-pregnancy diagnosis is most typical in the first four months after birth.
There are some important risk factors for postpartum depression. These fall into two categories: predisposition and situation. By far the biggest risk factor for postpartum depression is predisposition or prior experience of depression. If you’ve had episodes of depression before, they are more likely to crop up again in the pregnancy or postpartum period.
The other risk factors are largely about the situation. Some of these factors are modifiable, some are not. New parents who have less social support, who experience difficult life events around this time, or whose baby has medical or other problems are more likely to be depressed. And the baby itself can also play a role; people with babies who are poor sleepers are at greater risk for depression, almost certainly due to the fact that they, in turn, get less sleep.
Although postpartum depression is more likely in the birthing parent, due to hormonal shifts, it can also appear in non-birthing parents. Depression in new fathers is more common than many people think and certainly underdiagnosed. Many of the situational factors are similar, and the screening I discuss below is worth doing for all adults in the household.
How is postpartum depression diagnosed?
Ideally, every woman is screened for this using a short questionnaire at their six-week postpartum visit. The most widely used questionnaire is probably the Edinburgh Postnatal Depression Scale, though a few others are common. Here’s what it looks like:
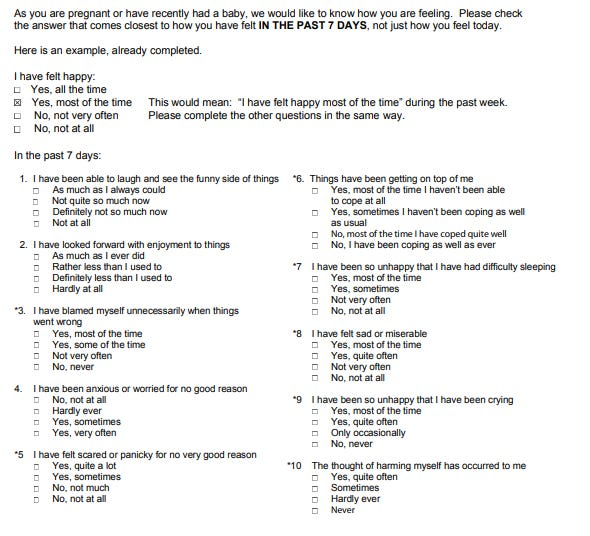
The scaling of it is simple: each question is scored from 0 to 3, with the worst category (the top one for most questions, the bottom for 1, 2, and 4) getting a 3. Doctors will typically use a cutoff of 10 or 12 as a signal of mild depression, and a value of 20 or more as signaling a more serious depression.
Evidence suggests that using this screening tool can be extremely effective. Researchers have shown improvements in detection (and therefore treatment) from using it, as much as a 60% reduction in depression a few months later.
If you are the birthing person, your doctor may give this to you at six weeks, and it is possible that your child’s pediatrician will, as well. This screening is good, but it is probably not sufficient. It captures only a point in time, and it focuses only on the birthing person, not any of the other adults in the household. In my view, it would be a good idea to have every adult in the household do a depression screen a few weeks after the baby is born, and then periodically after that. This could pick up more cases early and accelerate treatment.
How is postpartum depression treated?
Treatment for postpartum depression proceeds in stages. For mild depression, the first approach is to try to treat without drugs. There is some evidence that exercise or massage can be helpful or, perhaps most important, sleep. For new parents in particular, lack of sleep can be a huge contributor to mild depression. This shouldn’t be that surprising. Even when you don’t have an infant, if you have a few nights of poor sleep, it can be hard to enjoy things. Now add together many, many nights of interrupted sleep; it’s not surprising this could contribute to emotional exhaustion and depression.
Obviously, it is hard to treat lack of sleep when you have a newborn. But there are ways to try to improve things a little. Get help for a night or two — or more — from a grandparent or friend. Hire a nighttime doula if possible. Divide the night duties with a partner so you can each get at least one uninterrupted stretch of sleep. It may be helpful to remind yourself that addressing depression is valuable for your baby, too, not just some kind of selfish personal indulgence.
Beyond sleep, some type of cognitive behavioral therapy or other talk therapy is a usual first-line treatment for many people. This focuses on reframing negative thoughts and focusing on positive actions.
For more severe depression — sometimes defined as a score above 20 on the standard depression screen — antidepressants are more widely used. Although antidepressants are passed through breast milk, there is no evidence of adverse consequences. This means there is no need to choose between getting help and breastfeeding.
What about other postpartum mood disorders?
Much of the literature and popular discourse focuses on postpartum depression. But not all postpartum mental health issues take the form of depression. Postpartum anxiety is also common. Many of the symptoms are similar to postpartum depression, and indeed, it is common to diagnose postpartum anxiety using the same screening tool. But women with postpartum anxiety also tend to find themselves fixated on terrible things that could happen to the baby, unable to sleep even if the opportunity is there, and engaging in obsessive-compulsive behaviors around infant safety. This can be treated with therapy or, in more severe cases, with medication.
With anxiety, it can be hard to know where the line is between normal parental worry and obsessive worry. If anxiety is interfering with your ability to enjoy spending time with your baby, if it is occupying all your thoughts and preventing you from sleeping, that is over the line.
Less common but much more severe is postpartum psychosis. This affects an estimated one to two in 1,000 women and is much more likely to develop in women with a history of bipolar disorder. Postpartum psychosis usually manifests in hallucinations, delusions, and manic episodes. It will very likely need inpatient treatment and should be taken extremely seriously.
Closing thoughts
There are many issues in the pre-pregnancy, pregnancy, and post-pregnancy world that we do not talk about enough. When I was writing about pregnancy, the thing that struck me in this category was miscarriage. So many women have had miscarriages, yet they are rarely talked about — until you have one, and then it turns out many women you know have also miscarried.
Postpartum mental and physical health have the same pattern. You have a new baby — shouldn’t you be happy and feeling great? When people ask how you are, everyone wants to hear, “The baby is great! We’re so thrilled!” Not “I’m depressed and anxious, and I’m dealing with third-degree vaginal tears.” The fact that these things are not talked about makes many of us feel like we are the only ones dealing with them, or that we should just get over it.
This simply isn’t true, and I think the more we talk about this, the more we do a service to other new parents. It’s time to have a more honest conversation.
The bottom line
- Postpartum depression and/or anxiety are common and can show up anytime from the first few weeks after birth to many months later. Postpartum psychosis is less common but much more severe, will likely require inpatient treatment, and should be taken extremely seriously.
- If you are suffering, please get help. Reach out to your OB or a therapist if you have one, or see other resources, including Postpartum Support International.













Log in
I want to add something to this: you may find that your OB is not sufficiently helpful. You may find that your therapist or psychiatrist are unprepared for the specific condition of postpartum depression. You don’t have to accept this. If the professional you reach out to is not warm and caring, or does not make sure to see it through with you until you find the care that actually makes you well, you have the right to advocate for yourself and find a new care professional.
I absolutely agree. My OB was never helpful. Look for a reproductive psychiatrist in your area or a psychiatrist who specializes in women. Made all the difference for me after I was diagnosed with PPA/PPD after my first baby. I had three children now and have been under phenomenal care to prevent relapse.