



In vitro fertilization, or IVF, is the most effective fertility treatment for individuals and couples trying to conceive. There are many different types of IVF, but I’ll focus on the basics of autologous IVF, or IVF using your own eggs. This is distinct from reciprocal IVF (using a partner’s eggs) or IVF using donor eggs, though there is a lot in here that also applies to those situations.
IVF is fairly common. According to the CDC, about 2% of all infants born in the U.S. are the result of IVF, and that percentage is projected to increase given the prevalence of infertility, as well as trends of delayed childbearing.
It’s important to recognize that not everyone’s experience of IVF is the same. Your IVF journey may not look or feel exactly like another person’s. Many people say that the process feels overwhelming and difficult. I have also taken care of many patients who felt affirmed and satisfied by their IVF process. However you feel, know that you are not alone and there is support for you.
To help you understand IVF, we’ll cover:
- What is IVF?
- What are common symptoms of IVF?
- How successful is it?
- When is it time to consider IVF?
- How can you prepare?
This is a general overview for anyone trying to conceive or navigating infertility and fertility treatments so you can have more-informed conversations with your doctors.
What is in vitro fertilization (IVF)?
Broadly speaking, IVF is a procedure where eggs are extracted from the body, fertilized in a lab, grown into embryos, and one or more embryos are put back into the uterus to implant. But to completely understand the process, you have to start with the menstrual cycle.
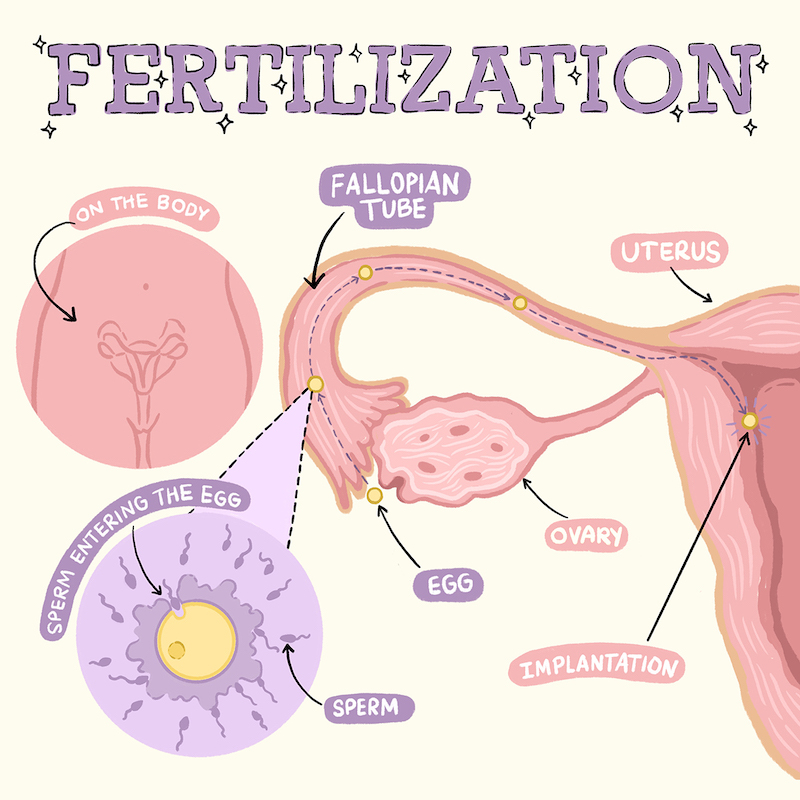
As a reminder, in a normal menstrual cycle, the body releases a pool of eggs and one (sometimes two!) of those eggs is randomly selected to grow in a fluid-filled sac called a follicle. This egg is released during ovulation and can be fertilized by sperm. The rest of the eggs that were released but did not grow end up dying, and the whole process starts again the next cycle if you do not become pregnant.
The first step in an IVF procedure is to encourage as many eggs as possible (rather than just one or two) to grow in follicles so they can be retrieved before you ovulate. This part is called stimulation. This is done through hormone injections, administered through a shot, and regular monitoring through ultrasounds and blood work.
IVF cannot create new eggs; it can only work with what your body has released. That means if you have a low egg count or a higher proportion of lower-quality eggs because of age, IVF cannot fix that. Particularly if you have concerns about egg quality, you will often hear IVF referred to as a “numbers game” — the idea being that by making a large number of eggs available to be fertilized, the odds of finding a “good” egg are increased.
All of this also means that you are not using up your eggs any faster or slower than you would have otherwise; IVF is simply “recruiting,” or growing, eggs that would have otherwise died.
In order to retrieve the eggs, a vaginal ultrasound is done, very similar to the ones done during monitoring but this time with a small needle attached. The needle pokes through the vaginal wall to where the ovaries are, and the fluid in each follicle is drained. An embryologist then looks at the fluid underneath a microscope to isolate the eggs. Rarely, we are not able to safely access the ovaries vaginally, and in these cases we may try to access them through an ultrasound on the abdomen. Still, no incisions are made. We always prioritize safety even if that means leaving eggs behind. These procedures are done under anesthesia, so you are asleep and shouldn’t feel anything.
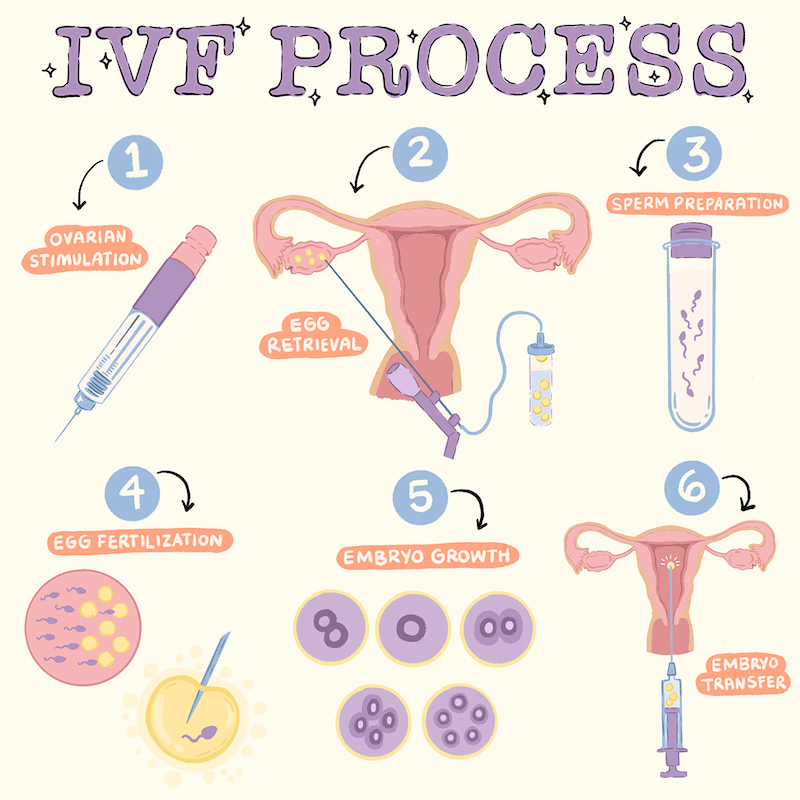
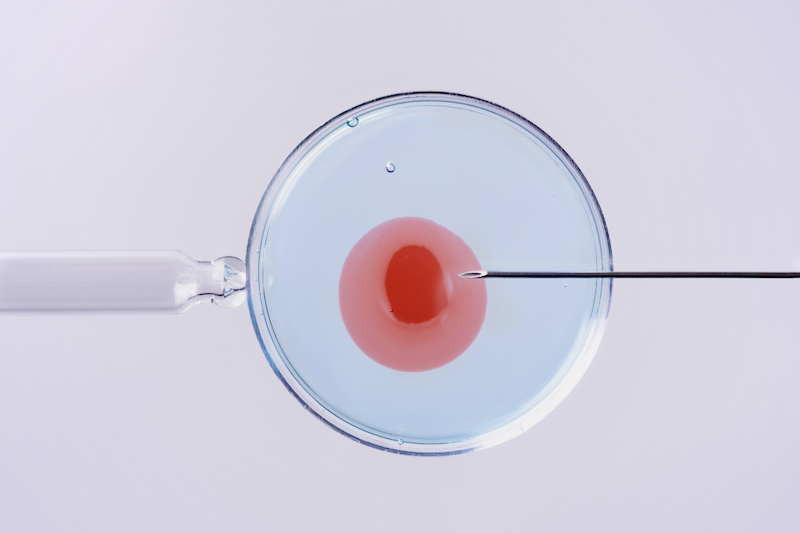
The next step happens in a lab; the eggs are combined with sperm to create embryos. There are two ways that sperm can be combined with eggs: either by “conventional” insemination, which is putting an egg in a petri dish with sperm and letting the sperm “compete” to fertilize the egg, or by intracytoplasmic sperm injection (ICSI), where a single sperm is injected directly into the egg.
Those embryos are then transferred back into the woman’s uterus during a separate medical procedure. Typically one embryo is transferred at a time, though the number of embryos transferred at a given time is dependent on your age, the quality and genetics of the embryos, and your reproductive history. So if you’re in your 40s and have embryos that have not been genetically tested, your doctor may recommend transferring more than one at a time.
The embryos can be transferred during the same cycle as you undergo stimulation (fresh transfer) or they can be frozen and then thawed at another time to be transferred (frozen transfer). Before an embryo transfer, you can also choose to have the embryo(s) genetically tested for specific illnesses that you carry or that run in your family or to make sure the embryos are euploid (have 23 pairs of chromosomes). In these cases, the results take a few weeks to come back, so the embryos are frozen in the meantime and you would later undergo a frozen embryo transfer.
The embryo transfer is much more straightforward than the retrieval. For the transfer, a small catheter is placed inside the uterus and the embryo is “loaded” into another, smaller catheter that fits inside the first one while it is in place. This is all done while you are awake and feels very similar to intrauterine insemination (IUI).
Whereas IUI simply bypasses the vagina and cervix, IVF is involved in every step of the fertilization process. While it is the most effective treatment we have for many infertility cases, that effectiveness unfortunately comes with a lot of tradeoffs; it is a very physically demanding, time-intensive, and costly process.
What are common symptoms of IVF?
Let’s break this down into the three different parts of IVF: stimulation, retrieval, and transfer. Keep in mind that everyone’s experience is different.
Because IVF medications are purified versions of hormones your body is already making, many people do not have negative side effects. Most of what is felt during the stimulation is from the medications doing exactly what we want them to do: encouraging as many eggs as possible to grow. This can make your pelvis feel very “full,” and you may also feel bloated. It can take six to eight weeks after the retrieval for your ovaries to completely go back down to their normal size, but you should feel better after your retrieval.
After the retrieval, you may feel some vaginal soreness and pelvic cramping, both of which should be manageable with over-the-counter Tylenol and ibuprofen. Because the retrieval is considered a surgery, it does have the risks of bleeding, infection, and damage to the bowel and bladder. All of these are extremely rare, but if you find that your pain is not controlled by Tylenol and ibuprofen, this may be a sign of a complication and you should reach out to your practice right away. Similarly, your bleeding should be no more than spotting, so if you are soaking through pads, that is another reason to contact your practice. You will also be a little tired and groggy from the anesthesia, so you should plan to take the day of the retrieval off from work.
The most dangerous complication of IVF is something called ovarian hyperstimulation syndrome, or OHSS. Severe OHSS is now very rare thanks to more intentional medication dosing and monitoring, but in the worst cases it can mean hospitalization. Your doctors will let you know if you are at high risk of developing OHSS, but if you find that you are gaining a significant amount of weight after a retrieval, having difficulty urinating or breathing, or having nausea or vomiting, please let your practice know right away.
How successful is IVF?
IVF is a somewhat unique area of medicine where you are putting in a lot of resources toward a positive outcome. As a result, there is a lot of focus on success rates. Unfortunately, this is another area where your specific situation is needed to get an accurate estimate.
In general, the single most important factor in determining IVF success is the age of the woman who is undergoing IVF; the older the age, the lower the chances of success. This is mostly because the quality of eggs, or their ability to lead to a healthy baby, go down with age, although the number of eggs available also decreases and that plays an important role.
Along those lines, ovarian reserve testing — anti-Mullerian hormone level (AMH, a hormone produced by eggs), follicle-stimulating hormone (FSH)/estradiol levels (hormones that your brain produces to help your ovaries make eggs), and antral follicle count (AFC, a count of the eggs your body released in a given cycle) — is also predictive of success because these tests can give a sense of how well you are expected to respond to IVF stimulation and how many eggs you can expect from a given IVF cycle. Other factors, such as if donor sperm is being used and chronic medical conditions, are also extremely important.
With this information, you can use one of the many online calculators that predict IVF success. These calculators are based on data on IVF outcomes submitted to either the CDC or the Society for Assisted Reproductive Technology on patients similar to you and give you an estimate of your chances of live birth after one, two, or three IVF cycles. Keep in mind that these estimates are if you transfer all of the embryos resulting from those three cycles.
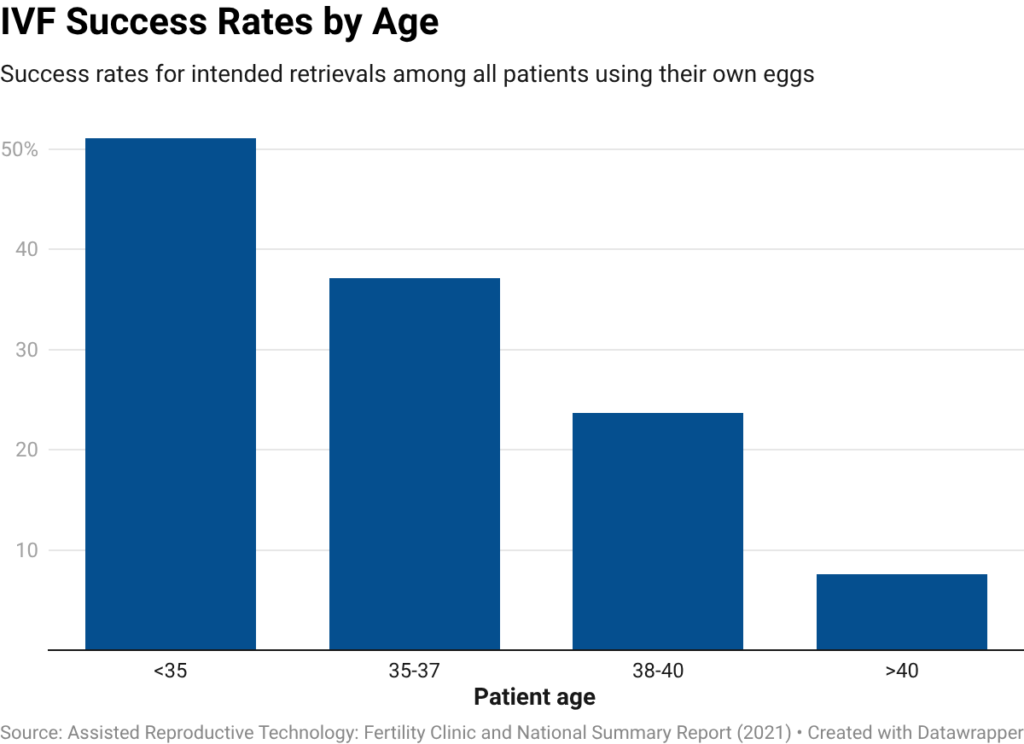
The CDC reports annually on national cumulative IVF outcomes by age and whether or not the patient’s own eggs are being used. You can see the results from the latest report in the graph below. For women younger than 35 using their own eggs, the success rate was 51%, and for women 40 and older it was about 8%. However, the pregnancy rate after transfer of a euploid (or genetically normal) embryo after IVF is typically between 60% and 65%.
Finally, you may have heard that you should be looking at each clinic’s success rates. When comparing success rates between clinics, remember that certain clinics may be more willing to take on cases with lower chances of success. These success rates should be used as a conversation starter with your fertility provider.
When is it time to consider IVF?
There are two paths that often lead couples to IVF.
For some, their fertility journey starts with IVF. This can occur when people are hoping to prevent passing on a specific genetic condition to their children (such as sickle cell disease or cystic fibrosis); if both fallopian tubes are blocked; and if neither partner has a uterus or is able to carry a pregnancy (in which case we would use IVF with a gestational carrier). Some couples pursue IVF immediately with advanced maternal age and a desire for multiple children.
The second path is one you are probably more familiar with. Many individuals and couples pursue IVF after initially trying to get pregnant through sex or after more conservative fertility treatments like IUI. If you fall into this category, it can be tough to determine when moving to IVF is the right decision for you.
One thing that can help is being realistic about how IVF may be able to help, given your fertility issues. I like to think of IVF as controlling for everything we can possibly control. So if there is anything along the path between ovulation and implantation that is an issue for you or your partner, or if there is an issue there that we just don’t have good ways of testing, IVF can possibly address or shed some light on that. This is also why you may sometimes hear IVF referred to as a very expensive diagnostic test; sometimes the issue ends up being something we can only diagnose in a lab, like total fertilization failure, which is when none of the eggs fertilize. If this happens, it can be really helpful to have an appointment already scheduled with your provider for after your IVF cycle to go over next steps.
How can you prepare?
In preparing for IVF, it is important to keep in mind that it is physically demanding and time-intensive.
IVF involves giving yourself hormone injections daily for a period of about two weeks. During that time, you will be coming into a fertility office for ultrasounds and blood work very frequently — every two to three days in the beginning of those two weeks, and daily toward the end. All of this is to see how your body is responding to the medications, adjust your doses, and time your retrieval.
You will usually not get much more than two or three days’ notice before your egg retrieval, which is typically done under anesthesia, so you will need to plan to take a full day off work. The short notice is because your retrieval is timed for when you have the maximum number of mature eggs, and that can be difficult to predict ahead of time.
So you should plan to do IVF during a time when you are not planning to travel and have a lot of flexibility in your schedule. If that’s not possible, you should plan to do IVF during a time when you can take about two weeks off from work.
It’s also important to identify support systems prior to starting an IVF cycle. As mentioned, IVF can be tough. It can also start to feel all-consuming, especially if you do not have people besides your partner (if applicable) to talk things through and activities to take your mind off what you are going through. Think through who you want to tell that you’re going through the process, if you want to join any support groups, and if you want to work with a mental health provider during this time.
Prior to starting an IVF cycle, your provider is going to want a few tests to help develop your IVF protocol, or the combination and dosing of the medications you’ll take during your IVF cycle. Some protocols involve prep work during the cycle before you start IVF, so keep that in mind when considering your timeline.
The bottom line
- IVF is the process of extracting eggs from the body, fertilizing them in a lab, growing them into embryos, and implanting the embryos back into the uterus.
- While IVF is the most effective treatment we have for many infertility cases, that effectiveness unfortunately comes with a number of tradeoffs; it is a very physically demanding, time-intensive, and costly process.
- IVF involves daily hormone injections, frequent visits to the doctor’s office, a minor surgical procedure to retrieve the eggs, and another procedure to implant an embryo back in the uterus.
- The single most important factor in determining IVF success is the age of the woman who is undergoing IVF; the older the age, the lower the chances of success. You can use one of the many online calculators that predict IVF success.
- Before going through IVF, consider your fertility goals, develop a plan for support, and plan to do IVF during a time when you are not traveling and have flexibility in your schedule.













Log in
I was a bit jarred to read the comment that ivf has not been found to improve the rate of live birth for people with recurrent miscarriage. Most major ivf clinics advertise they can help with recurrent miscarriage. Is there data that something can help the live birth rate for people with recurrent loss? Is it better to just try until one pregnancy is successful?
It seems odd to me that the columnist thinks that because the hormones are purified versions of what your body already makes, that means side effects are minimal. Birth control is basically the same and also can have a lot of side effects. I definitely had much stronger mood swings from my egg developing meds than I did from regular birth control or from being on nothing. The ovarian ultrasounds are also really uncomfortable.
Sometimes I think the framing of describing IVF as “all-consuming” and “overwhelming” makes people more scared of the process than they need to be. Yes, IVF does take a good bit of time, but I was actually surprised that the injections only lasted about 10 days. And the appointments, while yes many, can be made early in the morning before work and are very brief.
IVF can certainly be emotionally draining (and yes, financially draining), but making women feel like the process itself is also insurmountable isn’t helping anyone take rational steps toward the healthcare they need.
On the flip side, I was not at all prepared for how all-consuming and overwhelming the process would be, and I ended up going on Zoloft to help manage my anxiety. So I think it goes both ways!
And IVF is not just the egg freezing! If you do a transfer is at least 10 weeks of painful progesterone shots!
and the great irony of complaining about IVF being “all-consuming” and “overwhelming” as if pregnancy and childbirth isnt😭 in fact theyre almost guaranteed to be 10x worse
everything has tradeoffs!
Hi! Having gone through 2 egg retrievals and with many friends who have also been through IVF with similar experiences, I take serious issue with this sentence: “After the retrieval, you may feel some vaginal soreness and pelvic cramping, both of which should be manageable with over-the-counter Tylenol and ibuprofen.” It isn’t. It’s very painful. This makes it sound like light period pain. Nope. This reminds me of the horrifying podcast series “The Retrievals” and echoes a long and deep minimizing of women’s pain–especially in relation to fertility–by the medical establishment and society at large. If you are going through IVF and your doctor represents it this way, get a different doctor. Thankfully, I was at a major research hospital with amazing practitioners who without asking prescribed a few pain meds for the first 1-2 days. And even then all I could do was lay on the couch for at least 24 hours. Look, IVF is amazing and I have 2 beautiful kids because of it. But let’s not pretend it’s not a giant LITERAL pain to go through.
Oh also it’s not just “considered” a surgery. It is a surgery. You’re under general anesthetic (or should be, and if you’re not, get a different doctor ASAP). Your internal organs are pierced. Your ovaries are pierced again and again and again, for each egg. It’s a surgery.
So sorry that you experienced so much pain, the whole IVF process can be mentally and physically brutal. FWIW I also went through two retrievals and was at risk for OHSS both times, and for me the experience was as described in the article- no pain and just some soreness that I took advil for on day one. Not saying I’m the norm and I know friends who went thru IVF who had different physical reactions to each step of the process than I did, so I think it can really vary.
Same. It really was like period pain for me and didn’t last very long. I did get a sudden and very extreme skin reaction a few days later where my whole face was covered in pus filled spots. Everyone is different and while you should be made aware that you might have an extreme or unusual reaction, we also shouldn’t make out like those are typical.
I am so sorry you had a painful experience! I would like to add that experiences can definitely vary – I went through 10 retrievals, and experienced no pain or cramping.
I am so glad ParentData has created this newsletter. IVF is an area where even doctors don’t seem to agree on the meaning of what limited data we have regarding certain practices (the value of CoQ10, the use of Omnitrope, when to do uterine testing for failed embryo transfers, etc.).