






In many ways, a vaginal birth after cesarean (VBAC) is just like any other vaginal birth: your labor begins spontaneously or is induced, you progress to complete dilation, you push, and a baby is born.
In other ways, a VBAC is incredibly special. As a midwife, I’ve found that mothers who thoughtfully weigh the risks and benefits and choose to pursue a VBAC — despite the uncertainty — often experience their vaginal birth as deeply redemptive, meaningful, and empowering.
Unfortunately, the ability to attempt a VBAC is limited for many in the U.S. Surveys show that about half of people with a prior C-section would like to give birth vaginally in a future pregnancy, but of those, only around half are given the option. Many hospitals and physicians refuse to attend a VBAC, offering only the option of a repeat C-section. Access varies widely by region, and if you strongly desire this option, you will often need to be a staunch self-advocate, seek out supportive healthcare providers, or travel to a more distant hospital.
Assuming you have a choice between a VBAC and a planned C-section, it is reasonable and valid to consider both. Successful VBAC offers the possibility of a shorter recovery, less pain, and a quicker return to caring for a newborn or other children. It can also help preserve the option of future pregnancies without escalating the risks associated with multiple cesareans. However, attempting a VBAC that ends in a repeat C-section is typically associated with more complications than a planned repeat C-section. In the end, many medical and personal factors come into play in making this decision with your healthcare provider.

What is a VBAC?
A VBAC is simply any vaginal birth that occurs to someone who has previously given birth by cesarean. (You may also see the initials VBA2C, which means they have given birth vaginally after two prior cesareans.)
While someone may plan on having a VBAC, birth is unpredictable. You may go into labor expecting to give birth vaginally, but for many reasons, your birth may ultimately end in a C-section. That’s why medical professionals typically use the term “trial of labor after cesarean” (TOLAC or LAC) when someone is pregnant or in labor. When still pregnant, a woman may plan TOLAC/LAC, but she has not had a VBAC until the baby is born vaginally.
How common are VBACs?
There are several ways to measure how frequently VBACs happen. One way would be to look at all of the women who have had a prior C-section and whether any of their later births happened vaginally. This is the overall VBAC rate, and in the U.S., the rate is around 14.2%. However, this is not the same thing as looking at women who went in initially hoping for a VBAC, since most people with a prior C-section plan to give birth this way again.
The TOLAC success rate refers specifically to the percentage of people who attempt a TOLAC and go on to have a vaginal birth. Among those who chose TOLAC in the U.S., the success rate was 74.7% in 2020, a noticeable increase over the 2010 rate.
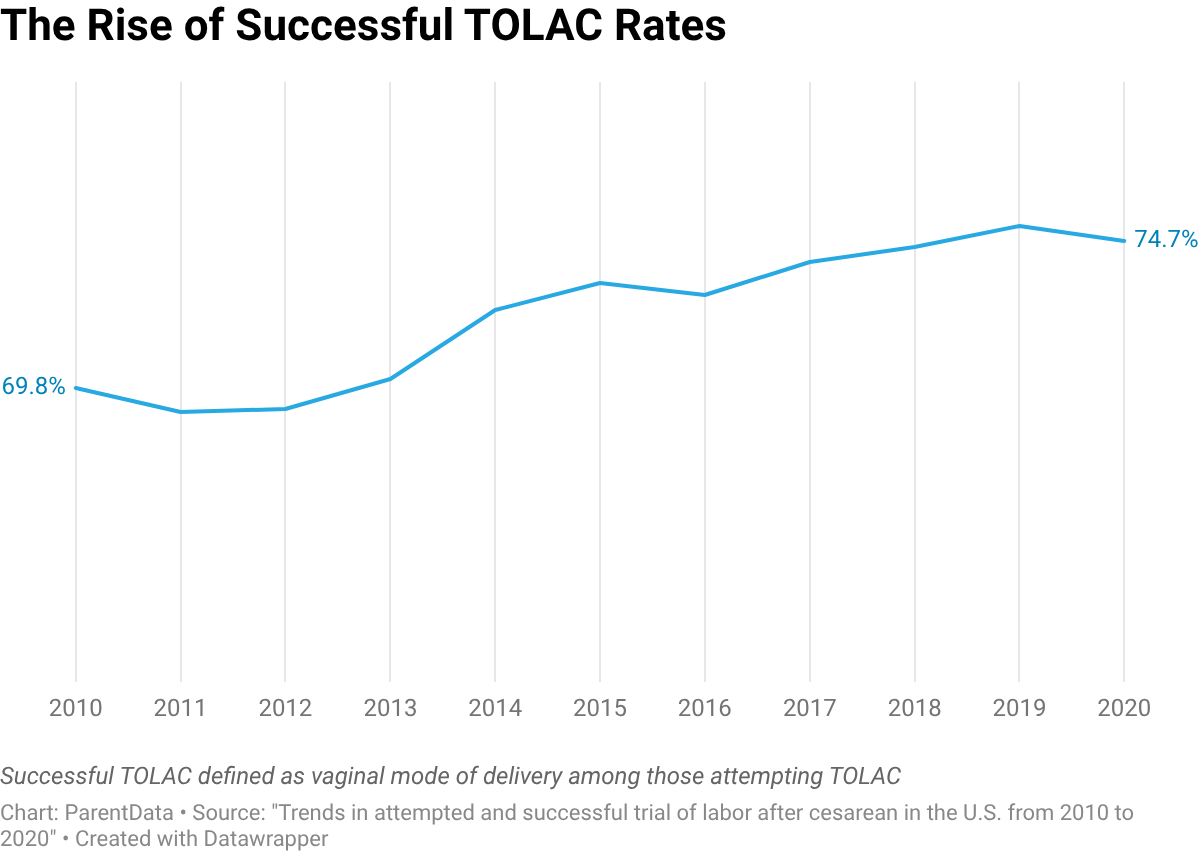
This is good news! It probably means that more people who want a VBAC are being encouraged and supported by their physicians and midwives during labor, and that facilities are growing more comfortable with VBAC as a way to safely reduce overall C-section rates.
What does prenatal care look like?
One key difference for people who want a VBAC is that discussions about birth planning should begin early. These conversations allow moms to understand their provider’s approach and hospital policies, helping ensure that their preferences will be respected if they choose to pursue a VBAC. Early discussion also gives you the time to seek a different provider if the current one is not supportive.
During early prenatal visits, the midwife or doctor should review the prior cesarean history and, ideally, obtain records from the previous birth in order to make personalized recommendations. Counseling typically includes a discussion of the risks and benefits of LAC versus repeat cesarean. There are very few absolute contraindications to LAC: previous vertical uterine incision (also known as “classical C-section”) and placenta previa, placenta accreta, or vasa previa. However, several factors are associated with a lower likelihood of a successful VBAC, including need for induction, an unripe cervix, advanced maternal age, obesity, a large baby, and a prior cesarean performed for failure to progress.
During labor, additional precautions may be recommended. First, the hospital may ask moms to sign a form acknowledging the risks and benefits of LAC and confirming their decision to proceed. Patients typically receive a complete blood count and type and screen, as well as an IV and continuous electronic fetal monitoring. Hospitals will also ensure that a surgical team and operating room are immediately available.
Pain relief during labor is up to you. Some providers recommend epidurals, as it is helpful if an emergency C-section is needed. However, it is not required, and some moms prefer to avoid epidurals to support labor progress. There’s no strong evidence that getting an epidural lowers your chances of a successful VBAC. In fact, studies show similar — or even higher — VBAC success rates among those who use epidurals during labor. The choice to use an epidural is best understood as a comfort preference rather than a factor that highly influences whether a VBAC will be successful.
What are the risks and benefits?
The most serious risk of LAC is uterine rupture, which occurs in less than 1% of labors after cesarean. This rare but life-threatening emergency happens when the wall of the uterus tears, usually at the site of the prior C-section. If rupture occurs, an emergency C-section is required to protect the life of the baby and prevent severe maternal hemorrhage. Rapid access to a skilled surgical team is critical for a good outcome.
A study of 36 uterine ruptures in Utah — a state with very high TOLAC and VBAC rates — showed that outcomes were good for babies delivered within 18 minutes and poor for babies delivered more than 30 minutes from the time of uterine rupture. Major medical societies like ACOG recommend against home birth after cesarean (HBAC) for this reason, suggesting that moms should only attempt VBAC in facilities capable of performing emergency cesareans.
Thankfully, both TOLAC and repeat C-sections have very low absolute risk of death or serious injury to mother or baby.
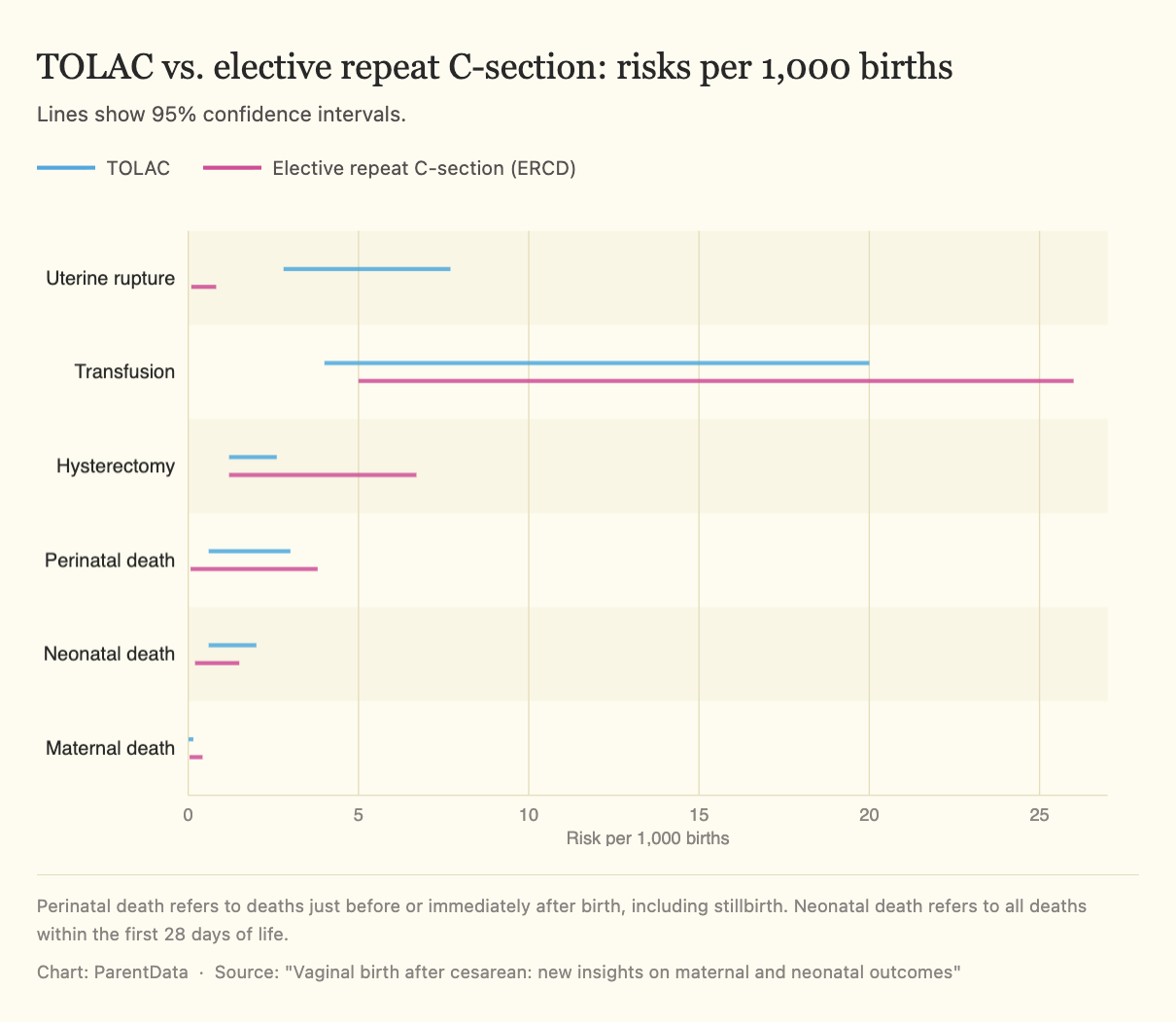
While uterine rupture is understandably frightening, it’s important to remember that repeat C-sections also carry some risks, many of which can be avoided if a VBAC is successful. These include increased risk of infection, excessive bleeding, blood clots that can travel to the lungs, injury to surrounding organs, longer recovery times, and complications in future pregnancies, such as abnormal placentation and placental abruption. These risks increase with each subsequent C-section, so people who plan to have future pregnancies often consider LAC to be a safer option for their long-term health.
I also see meaningful psychological and emotional benefits to VBAC. Many mothers describe their prior cesarean as traumatic — sometimes because it felt unexpected or rushed, and other times because they didn’t fully understand why it was necessary or didn’t feel included in the decision-making process.
While it’s not possible to change the circumstances of a prior birth, planning and pursuing a VBAC often gives moms a real sense of agency. Even when a TOLAC does not result in a vaginal birth, the experience of being heard and given options in labor is really valuable to mothers.
How to prepare for a VBAC
As a midwife, I care deeply about women having access to VBAC, but I don’t have a crystal ball to predict exactly how pregnancy, labor, and birth will go. What I can do is review the risks and benefits, provide guidance, and support whatever decision a mom makes. Mostly, I want people who have had a prior C-section to remember they are a pregnant person like any other.
Here’s what I recommend if VBAC is important to you.
Find the right provider
You should bring up VBAC early and often with your doctor or midwife. Make sure that the hospital where your doctor or midwife attends births supports VBACs, as many do not. Ask specific questions such as do you attend many VBACs? and is VBAC common at the hospital where I will give birth? An honest provider should tell you early on if VBAC is not part of their practice.
Some doctors and midwives use a VBAC probability calculator that estimates the likelihood of success based on factors such as age, weight, height, and obstetric history. In my own research, I found that the calculator significantly underestimated VBAC success for women who were overweight or obese and for those with no prior vaginal births. It only considers patient factors — but not important factors like overall hospital cesarean rates or provider type (midwife or physician), both of which can influence VBAC success. For these reasons, I recommend against being discouraged or dissuaded from attempting VBAC based on this calculator, and I do not regularly use it in my practice.
It’s helpful to ask detailed questions about contingency planning as well. It’s not just about whether your provider “allows” VBAC, but how they approach common scenarios that can come up toward the end of pregnancy — like going past your due date or developing a medical complication like pre-eclampsia that requires induction. Understanding their typical recommendations in these situations can give you a clearer picture of how supported you’re likely to be if your pregnancy doesn’t follow a straightforward path.
Some providers are very supportive of TOLAC plans early in pregnancy but may become more cautious as delivery approaches — especially if you go past your due date or if concerns arise about things like the baby’s size. While these factors may affect the likelihood of VBAC success, they are not, on their own, contraindications to attempting VBAC. Ask questions like what do you recommend to moms who go past their due dates and still want a VBAC? and if induction is recommended because of a medical reason, are you willing to induce labor even though I’ve had a prior C-section?
These conversations will help you understand whether your provider and birth setting’s policies align with your desires and give you time to seek another doctor or midwife if they do not.
Consider hiring a doula
Consider hiring a doula to provide additional support during labor and to help ensure your wishes are respected. It can also be helpful to talk openly with your partner or other support people about why VBAC matters to you so they can advocate alongside you.
And while it may be tempting to consider home birth — especially if you have lingering negative feelings about your prior cesarean — I think it is preferable to find a supportive hospital-based doctor or midwife, as TOLAC will always be safest in a setting where emergency care is immediately available. While a study of planned home birth after C-sections showed high VBAC success rates, it also found an increased risk of infant mortality.
Know that you don’t have to make the decision right away
Many people still feel uncertain about TOLAC late in pregnancy, and sometimes a “wait and see” approach makes sense. I’ve cared for people who scheduled a 39-week repeat cesarean but went into labor beforehand and had beautiful VBACs, and others who planned a TOLAC but chose a repeat cesarean after 41 weeks because they didn’t want to face a long induction. While it’s helpful to have thought about your preferences and plans, you are allowed to change your mind at any point, as long as you have found a supportive provider and birth setting.
At the end of the day, you should surround yourself with people who believe in you, respect your preferences, and are prepared to keep you safe. That combination is what matters most!
The bottom line
- Vaginal birth after cesarean (VBAC) can be a safe and meaningful option for many women — but access depends heavily on where you live and who provides your care.
- If VBAC is important to you, finding a truly supportive provider and birth setting early in pregnancy is one of the most important steps you can take.
- Attempting labor after cesarean (LAC) carries a small risk of uterine rupture, while repeat cesareans may carry higher risks of surgical complications and risks in future pregnancies.
- There is no single “right” choice — the best decision is one that aligns with your preferences, your medical situation, and the level of support available to you.












Log in
One interesting thing about this study though is that one of the authors commented that 3 of the 5 neonatal deaths in the TOLAC group were unrelated to prior cesarean scar- a cord prolapse, twin and surprise breech. Does this change how you would interpret the safety of an HBAC in this study?
https://lamaze.org/Connecting-the-Dots/Post/planned-home-vbac-in-the-united-states-2004-2009-interview-with-study-author-melissa-cheyney-phd
Describing VBAC as feeling “redemptive” seems to me to be a bit irresponsible and problematic. It might feel that way, but isn’t that a problem? Shouldn’t we also be trying to reduce the stigma that having a cesarean is somehow less than having a vaginal birth? There are other moments here too that imply that VBACs mean that doctors are “supportive” and moms have “agency” (“planning and pursuing a VBAC often gives moms a real sense of agency”) — but it’s also incredible supportive for a doctor to tell a mom that she isn’t a good candidate for a VBAC when she’s not, and there’s agency in a mom having a cesarean when that’s what’s best for her and her child. Articles with this kind of language inherently play into an unnecessary binary between cesareans as medical “interventions” that turn a mother into a passive, non-laboring person, and vaginal birth as “supportive” medical care that is “natural” and empowering — when we should see both as incredible, life-supporting options.
I agree there is certainly agency in a mom being provided with accurate information and choosing of her own accord that repeat C-section is her best option. This is often the case–only about half of moms say they are interested in a VBAC and it is definitely true that some people are not good candidates. But the truth is, a lot of moms in the U.S. don’t get an option, which I view as very problematic. And when it comes to having a VBAC, there is a lot of literature showing that women do find it empowering and redemptive. This is probably because some women do not report feeling supported or having agency with their prior cesarean. In any case, yes, it is a good point that cesarean can also be a choice where a mom has agency and is being an active, rather than passive participant in her care!
Thanks so much for this post. As a woman just at the beginning of the journey for pregnancy #2 who’s planning a VBAC, this was useful context. My first cesarean felt like it was due to prodromal labor and years of accidental pelvic floor mistakes (I can’t believe I got to 9cm dilation with the bad habits I had creating so much tension). I feel like I’m in a much better position to deliver vaginally this time around
So glad you have the option to attempt VBAC and I wish you the best!