






I’ll acknowledge up front: this is an area I have done research on, but it’s not one I speak to from personal experience. This is why it feels so important to have other voices on ParentData who can speak to that experience. With my research hat on, though, I hope I can try to lay out what it means — in numerical terms — to say there is a crisis in Black maternal health.
Laying out data doesn’t provide answers, but with a better understanding of the problem, we can start to look for solutions, for policy, and through an individual lens.
I will caution here: some of this is scary, and it is never my intention to scare you. The risks we are talking about here are still very small, even though they are larger than they should be. But if this is not the moment for you to read this, please take care of yourself and come back to it another time.

What do we mean by maternal mortality?
I will start by getting us on the same page about what we mean when we talk about maternal mortality, since there are several ways to measure it. The World Health Organization definition, which the U.S. uses in calculating the headline maternal mortality numbers, is “death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.”
The two key components of this are the timing (during pregnancy or within 42 days of the end of pregnancy) and the exclusion of accidental or incidental causes. For the U.S., these data are produced based on comprehensive records of all U.S. deaths.
There are several other data sources that can be used to better understand these issues. The Pregnancy Mortality Surveillance System is a CDC-based surveillance system that uses death certificate information to further understand maternal deaths. These data include the possibility of deaths up to one year postpartum, reflecting pregnancy-related mortality. There is also data from CDC Maternal Mortality Review Committees that can provide further detailed information at the state or local level about the causes of maternal mortality.
What is the maternal mortality rate in the U.S.?
The most recent CDC data on maternal mortality rates is from 2024. The CDC reports these rates across racial groups and age groups; I’ve graphed them below. Again, to be clear, we are talking about rare events; these are quoted in deaths per 100,000 births. But what we see very clearly is that there are inequities inherent in these numbers by race.
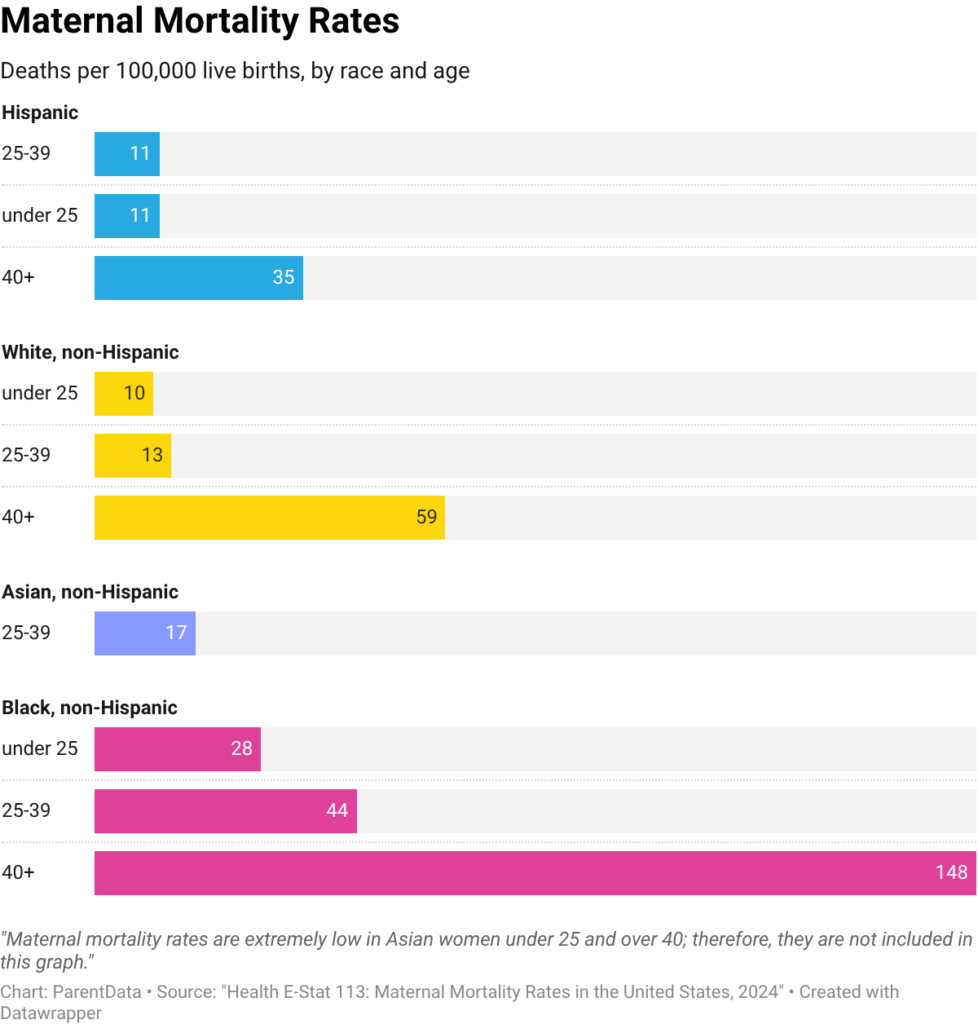
For Black women over 40, the mortality rate is 148 deaths per 100,000 live births. This is more than twice as high as that of white women in this age group. If we focus on the middle age group — 25 to 39 — the mortality rate for Black women is 44 per 100,000 — again, far higher than for white or Hispanic women in this age group.
The U.S., regardless of race, is an enormous outlier on maternal mortality. In Canada, the maternal mortality rate is 11 per 100,000. In Sweden, it’s five. This means that even for white women in the U.S., the maternal mortality rate is far higher than in our peer countries.
Black women in the U.S. have a maternal mortality rate comparable to Peru and Ecuador, despite the U.S. GDP being more than 10 times as high as in those countries.
What are the primary causes of maternal mortality?
In part because these numbers are scary, we want to find solutions. One way to move in this direction is to look for causes. What is really going on behind these deaths? I do not mean here root causes — Dr. Quantrilla Ard wrote about the role of racism in causing all of this — but proximal causes. If we know what is happening, that is one way to construct solutions.
It is sometimes challenging to code causes of death, since there is rarely just one cause. Because maternal mortality is so important, we can do better with Maternal Mortality Review Committees data, where doctors and researchers can read more deeply into the details of mortality events to better understand what happened. These data focus on deaths through the first year of life, so they are more comprehensive than the study of the first days.
In the table below, I’ve listed common primary causes of maternal death, both overall and for Black women, in 2021. The darker cells in the table represent the more common causes.
The details of this table may be a little hard to parse, but here are what I think are the key points. First, in 2021, COVID-19 was implicated in a large share of maternal deaths. These deaths were primarily among unvaccinated women during the Delta wave of the COVID-19 pandemic. This is likely specific to 2021; in the current time period, with the current COVID-19 variants, this is not a significant mortality risk.
Turning to the non-COVID causes of death, which are more likely to reflect the current risks, we find that in the population overall, mental health conditions are the leading non-COVID cause of death. This is a sobering reminder of very real postpartum mental health challenges.
For Black women, however, this isn’t the case. For that group, the leading cause of pregnancy-related death is cardiac conditions. Black women are also more likely to die of hypertensive pregnancy disorders (largely preeclampsia). This is important to know because many of these conditions have better outcomes when they are treated effectively. Take preeclampsia, for example. The risk of this condition is lower with proactive treatment during pregnancy (baby aspirin). If preeclampsia does occur in pregnancy, rapid diagnosis can lower the chance that something bad happens.
Both early treatment and rapid diagnosis will be possible with more monitoring and care. The fact that it is these conditions that are more manifest in Black women makes vigilance (and listening by providers) even more important.
How do income and BMI play a role?
In Dr. Ard’s piece, she alluded to the fact that income does not seem to be protective for Black women in terms of birth outcomes.
As a final data point here, let’s flesh out that statement. We know that, on average, Black women in the U.S. have lower incomes than white women. One suggestion that is sometimes made is that, perhaps, the differences in pregnancy outcomes are really about income and not about race.
This is a slightly challenging question since most data on mortality does not also have information on income. However, a team of researchers at Stanford and elsewhere merged data on maternal and infant health outcomes with income data.
What they find is that higher income does not lower maternal complications for Black women. In studying a variety of outcomes — maternal mortality, serious maternal health conditions, infant outcomes — they make two important observations.
First, although for non-Black women the risk of negative health outcomes goes down as their income goes up, this does not happen for Black women. Black women in the highest 10% in terms of income actually have serious complication rates similar to Black women in the lowest 10% in terms of income.
Second, the rate of serious outcomes for Black women across all income groups is much higher than the rate for low-income women of other races. Income is simply not protective here.
Finally, a note on BMI. Alongside income, another commonly argued explanation for racial disparities is differences in weight. On average, higher BMI is associated with greater maternal birth complications, and it is true that average weight differs across racial groups. However, this doesn’t translate to an explanation, for at least two reasons. First, it is difficult to draw strong causal (rather than correlational) links between BMI and maternal outcomes. Second, even if you thought there was a causal link, racial differences in pregnancy complications are not explained by these differences.
We can see this in data from New York City, which analyzes serious maternal morbidity by race and weight (see Figure 23). Black women have more complications at all weight levels. Notably, the serious maternal morbidity rate for underweight Black women considerably exceeds the rate for obese White women in these data. Put differently, while differences in underlying health conditions may play some role, they are not a full explanation by any means, and weight alone is certainly not a valid explanation.
I want to be clear. It isn’t that socioeconomic status and underlying health do not matter, or don’t relate to maternal health outcomes. Addressing these underlying societal inequalities should also be a policy focus.
But maternal outcomes for Black women are substantially worse than would be expected based on these characteristics. This suggests strongly that there is something in the experience of being a Black woman in the U.S. — in particular, a Black woman who grew up in the U.S. — which shapes these outcomes.
It is important that we continue to ask questions about the data and try to understand the underlying source of these differences in risk factors. As we do this, though, we cannot lose sight of the basic fact: the vast majority of maternal deaths are preventable, and it is unconscionable as a society to continue to sit by and watch this happen.
Closing thoughts
If you’re a Black parent, I hope that this is data you can bring into conversations with your partner, providers, and anyone else involved in your pregnancy care.
If you’re looking for ways to advocate for Black maternal health, there are a number of initiatives you can support, including the Momnibus. The Black Mamas Matter Alliance, the creator of Black Maternal Health Week, also released a detailed policy agenda that shares a vision for transforming data and research, reproductive health care, and more.
The bottom line
- There are several ways to measure maternal mortality, but the WHO defines it as the death of a woman during pregnancy or within 42 days of the end of pregnancy (excluding accidental or unrelated causes).
- CDC data highlights significant racial disparities in U.S. maternal mortality rates.
- Addressing these disparities through proactive care, vigilant monitoring, and rapid diagnosis can significantly improve outcomes, which emphasizes the importance of attentive medical teams tailored to these high-risk pregnancies.
- Higher income doesn’t protect Black women in the U.S. from severe pregnancy complications, unlike non-Black women. Additionally, differences in BMI or underlying health conditions cannot fully explain these racial disparities.
- The vast majority of maternal deaths are preventable, and it is unconscionable as a society to continue to sit by and watch this happen. There are several Black maternal health initiatives you can support, including the Momnibus.













Log in