






Is it okay to take Tylenol in pregnancy?
This is a question that has been coming up for years. Tylenol — generically, acetaminophen or paracetamol — is widely used in pregnancy, and the American College of Obstetrics and Gynecology says it is safe. However, over time, and especially more recently, concerns have been raised about possible links between use in pregnancy and neurological issues in children, notably autism and ADHD. The drumbeat of these claims has gotten louder as autism rates have gone up, and policy is focused on explaining that rise.
Let me start with the upshot here. The best data does not support this link. The increase in observed rates of autism over time must have other explanations, a main one of which is changes in diagnosis rates.
I will delve into the data below, but I want to start with the evidence that has led people to argue for such a link, providing the full context.

Why do we hear about an autism-Tylenol relationship?
There are a large number of papers and meta-analyses that link acetaminophen use in pregnancy to the development of autism and ADHD. One example paper from 2021 relies on data from six European countries and argues that the use of this medication in pregnancy increases the risk of ADHD from 4% to 5%. Their results for autism are of a similar size but less convincing.
A consensus opinion paper from 2021 — not a formal analysis, but a summary paper written by a set of experts — argues that the links in the data are enough to cause concern.
More recently, a paper from August 2025 provided a meta-analysis of studies on this link. They identified 46 studies, of which 27 showed significant positive links between Tylenol in pregnancy and neurodevelopmental disorder (others showed no results or a protective effect). In general, these studies show a link between frequent Tylenol use — often measured as more than 28 days over the course of pregnancy — and these outcomes. Occasional use generally does not show even a correlation.
It seems clear to me that there is a (small) correlation between Tylenol use in pregnancy and these disorders in children. However, correlation is not causation. In all of these studies, the women who take medication are different from those who do not, on dimensions like education, income, age, and other variables. Although the authors adjust for some of these differences, they cannot completely control for them. Categorizing education as “low,” “medium,” or “high” (as many papers do) does not, in fact, fully capture the differences in education across individuals. As I’ve written about before, studies that rely on this kind of observational data are subject to deep concerns.
People will sometimes say, “Sure, there are problems with these studies, but there are so many of them; doesn’t that make it more convincing?” The answer is: no. All of these studies have the same problem. There could be hundreds of them, but that wouldn’t make the problem go away! It would be better to have one more reliable study than a million problematic ones.
What does the best evidence say?
In April 2024, a new paper on this question was released, with better-quality evidence. The paper, published in JAMA, uses a sibling analysis to address this question. With this approach, authors compare outcomes (here, autism and ADHD) across siblings who have different exposures to acetaminophen while in utero.
I want to pause on that method. We all know that the “gold standard” for causality is a randomized controlled trial. In this case, such a trial is unlikely to occur for several reasons. A sibling analysis isn’t as rigorous as a randomized trial, but it’s a significant improvement over simply comparing across children. In short, this paper compares kids born to the same mother, where she took acetaminophen in one pregnancy and not the other. Because this analysis holds the mother constant, it can adjust for all of the mother’s characteristics — both the ones we can measure and the ones we cannot. This is able to effectively address many of our most significant concerns about a relationship being just a correlation.
The paper utilizes an enormous sample of people — 2.5 million births in Sweden, encompassing all singleton births in Sweden between 1995 and 2019. Women were asked about acetaminophen use several times during pregnancy, and diagnoses of children are measured in medical records (Scandinavian data is extremely complete).
The results: The authors first conducted a naive analysis – simply comparing across kids, without using the within-family comparison. When they do that, they find results similar to those in the existing correlational literature discussed above. There is a modest increase in ADHD and autism rates among children whose mothers were exposed to acetaminophen during pregnancy.
However, when they conduct their sibling analysis, they find that this result completely disappears. This is their most compelling analysis, and the result is: there is no relationship between acetaminophen exposure and these diagnoses. This is true when they measure any exposure and when they measure higher exposure amounts.
A second study, from September 2025, used a similar approach on over 200,000 births in Japan. These authors, again, show that in the simple analysis, they see a link between Tylenol use and neurodevelopmental diagnoses. But when they include sibling controls, the effect disappears. A third study, using Danish data, published in April of 2026 showed no relationship between Tylenol use and autism, either across or within sibling groups.
A fourth study, published in JAMA Pediatrics in early 2026, uses a dataset of 2 million births in Taiwan between 2004 and 2015. Similar to the Sweden and Japan studies, it measures whether children whose mothers had acetaminophen during pregnancy are more likely to receive ADHD or autism diagnoses. (Note: it relies on prescription data; over-the-counter use is less common in Taiwan.)
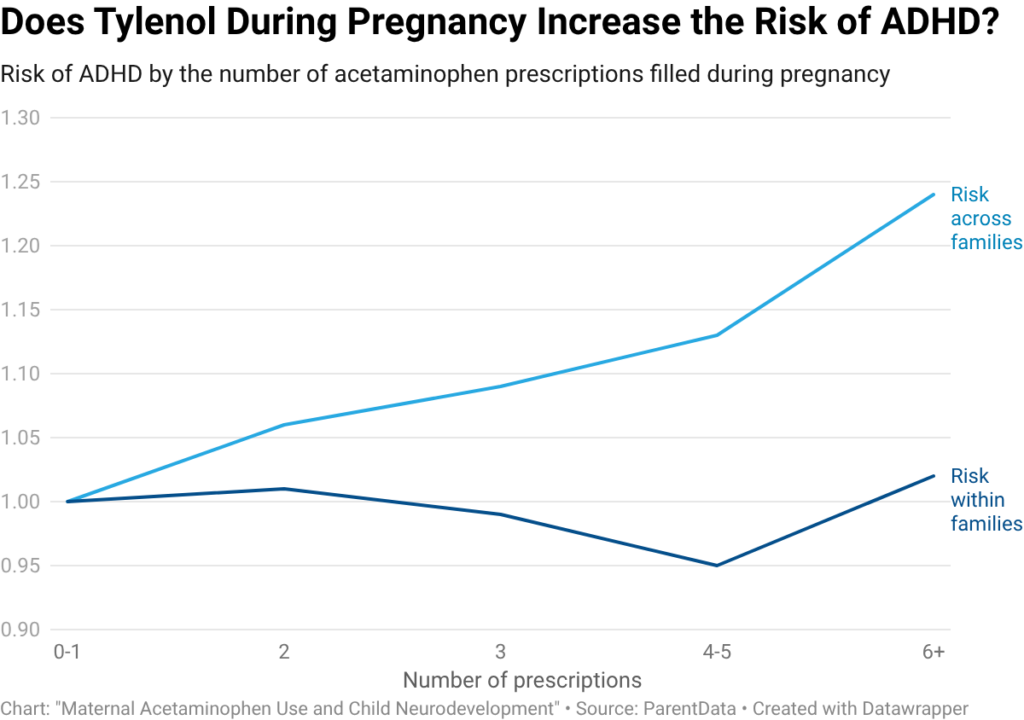
The results in this paper echo what we saw in the paper from Sweden. If you look at the relationship across families, there is a strong positive correlation between the extent of Tylenol exposure and ADHD diagnoses. However, when you look within families, the relationship disappears.
This paper also runs a second analysis, where they separate sibling pairs by which sibling was exposed. In this analysis, depending on whether the older or younger sibling was exposed, they see significant results in both directions. This suggests that even the sibling effects may be biased in complex ways, but do not detract from the overall conclusion that Tylenol exposure does not raise the risk of ADHD or autism.
Bottom line: Without sibling controls, higher exposure appears to be associated with more diagnoses. With sibling controls, higher exposure has no impact. This tells us both the answer (there is no link) and why other studies have found a different result (because their results are driven by other differences across people).
Explaining trends over time
These sibling data indicate no clear link between Tylenol usage in pregnancy and neurodevelopmental disorders. In addition, it is worth noting that even if you were to believe the results in the correlational data, the estimated impacts are extremely small. The results indicate that taking Tylenol for more than 28 days during pregnancy increases the risk of these conditions by perhaps one percentage point. Combined with the fact that the share of women taking Tylenol during pregnancy has been high and may have decreased somewhat over the past 20 years, it is not plausible that this would be an important cause of the enormous increase in autism rates over the past several decades.
Closing thoughts
When I started writing about pregnancy in Expecting Better, I spent a lot of time combing through the academic literature to find not just “what the data says,” but what the best data says. This often means discarding what seems like a substantial amount of evidence, some of which is published in reputable academic journals. Sometimes, though, that is necessary. We’ll make better decisions if we focus on the most reliable evidence.
And, in this case, that evidence says that Tylenol during pregnancy does not lead to an increased risk of neurodevelopmental disorders.
The bottom line
- There is no reliable data that suggests Tylenol during pregnancy leads to an increased risk of autism or other neurodevelopmental disorders.
- The studies that do show a connection could not replicate this connection across siblings, suggesting that their results are driven by other differences across people, not Tylenol consumption.
- If you need pain or fever relief during pregnancy, Tylenol remains safe to use.












Log in
Hi! Thank you for this. I’ve seen the question raised regarding whether these sibling studies adjusted for gender, but haven’t seen that question addressed anywhere. The idea being that since boys have a much higher rate of ASD and ADHD that potentially the comparing families where there are both male and female siblings, the females might be diluting the numbers as they seem to be less susceptible to these conditions in the first place. Any thoughts on this?
Are there any differences/studies with extra strength Tylenol?
Hi Emily,
I know I’ve asked about this before (here and on Instagram), but I haven’t seen you address it yet. Could you share your thoughts on paracetamol use in early childhood?
The research on pregnancy exposure is often described as low-quality or inconclusive, but the studies on early childhood use raise more concerning signals. Of course, neurological conditions are highly complex, with no single cause explaining the rise in cases – and increased diagnosis doesn’t account for everything. The indication seems to be that certain children may be especially vulnerable, which makes this even harder to assess.
If there’s even a small suspected link, parents deserve to be informed. At the moment, most of us are told that Calpol/Tylenol is “completely harmless,” which encourages frequent use – even for mild teething, or in large doses around vaccination time. At the same time almost all mainstream discussion focuses on pregnancy, not infancy or early childhood.
Because of this, many parents are convinced of its total safety, and raising questions about it risks being dismissed as “conspiracy theorising.” I’d really value your perspective on this – what does the evidence actually suggest, and how should parents think about risk?
Thanks!
These are questions people don’t like asking…I hate that you even asking opens you up for criticism.