






It is no secret that the issue of childhood vaccines is prominent in the national conversation. Robert F. Kennedy Jr. is well-known for his distrust of vaccines. States like Florida are banning vaccine requirements, while others are taking vaccine recommendations into their own hands, making guidance increasingly difficult for parents to understand. Even before this, in the wake of the COVID-19 pandemic, routine childhood vaccination rates have declined. Put simply: skepticism and misinformation are at an all-time high.
Most parents are asking me questions — often, nervous ones. Anxiety here is a natural impulse. We want nothing more than to protect our children, and already, sticking needles into them can feel scary. As a friend said to me once, My baby is just so small. Do they really need all these shots? Add to that external conversations about possible (but unsubstantiated) links to autism or vaccine injury, and it’s not surprising that people have questions.

Public health messaging doesn’t always fully answer the questions people have or provide enough information to navigate these choices. This article aims to close some of that gap.
I’ll go through each of the vaccines in the schedule in turn. I’ll explain the disease the vaccine protects against, the basic structure of the vaccine (when kids get them, how many shots), how effective the vaccine is, and whether there are any side effects to note. I then end with a few general questions about vaccines — how they work, why they’re important, and how we know they’re safe.
I’m focusing here on vaccines given through age 2. Many of these same vaccines are given as boosters later, and I’ve written elsewhere about one important vaccine, for HPV, which has a first dose typically between ages 9 and 11.
Buckle up: this is a long article, and one I hope you’ll save and share.
What vaccines does my child need?
I’m focusing here on the standard childhood vaccines, not on vaccines for COVID-19 and flu.
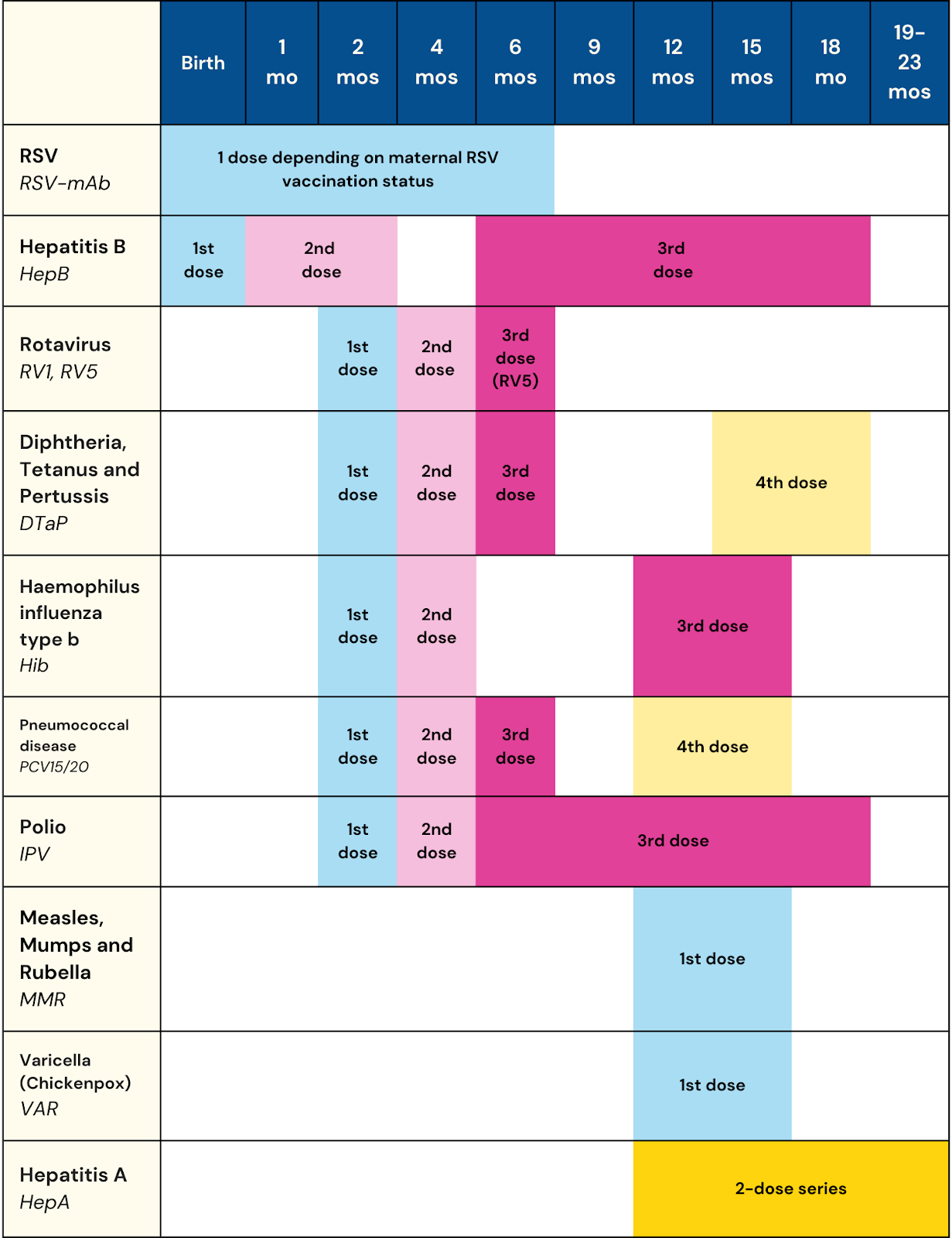
The graphic below shows the full set of vaccines that the American Academy of Pediatrics recommends for ages birth to 2. Below, I’ll discuss them in roughly the order that they happen.
RSV
- What is RSV? Respiratory syncytial virus (RSV) is a common respiratory virus characterized by runny nose, sneezing, and congestion. It is common in the fall, and most people will get RSV many times in their life. For older children and healthy adults, it is generally not dangerous. For infants and older adults, it can be very dangerous, because it can settle in the lungs and affect breathing.
- Vaccine basics: There are two ways to protect infants against RSV. Pregnant women can get an RSV vaccine during the third trimester of pregnancy. If that doesn’t happen, infants can get a monoclonal antibody shot at birth or anytime before eight months (this is not a true vaccine, as it delivers antibodies directly). Generally, you would choose one of these options, not both. This vaccine is only given in the first RSV season (i.e. fall/winter) for healthy infants and can be given shortly after birth.
- How well does it work? RSV is common. In infants under six months, the hospitalization rate for RSV is 14.7 per 1,000; RSV causes 100 to 300 deaths per year in children under 5 in the U.S. In trials and real-world settings, either version of this immunization seems to reduce the risk of hospitalization for RSV by about 80%.
- Additional notes: There was a concern when the vaccine for pregnant women was first approved about elevated rates of preterm birth. As the vaccine has rolled out, that has not been further supported in the data.
Hepatitis B
- What is hepatitis B? Hepatitis B is one of a number of hepatitis viruses that affect the liver. Acute hepatitis B infection can cause flu-like symptoms but is usually not serious. However, in a small share of cases, acute infection turns to chronic infection. This is asymptomatic but is a cause of liver cancer and liver failure. Hepatitis B is spread through bodily fluids, including from the mother at birth or in a day care setting. And babies and toddlers who are infected are much more likely to become long-term hepatitis B carriers than those who are infected older. This is why the vaccine is done in children.
- Vaccine basics: This is a three-dose series, with the first dose generally given at birth. This is done early because of the risk of transmission from the birth parent, if hepatitis B is undiagnosed. If you are sure you are not a hepatitis B carrier, some people will push the first dose to the two-month vaccines.
- How well does the vaccine work? There are approximately 13,000 acute hepatitis B cases per year in the U.S., mostly in adults. The vaccine provides between 80% and 100% protection against the hepatitis B virus.
Rotavirus
- What is rotavirus? Rotavirus is a virus that causes severe diarrhea in infants and young children. It can cause severe dehydration, which may have serious consequences. Rotavirus infection is ubiquitous — most of us will get it many times — but it is more serious in babies and young children. The vaccine targets protection in this age group. Before widespread vaccination, the disease caused an estimated 55,000 to 70,000 hospitalizations and 30 to 60 deaths of children per year.
- Vaccine basics: This vaccine is a two-dose series, typically given at two and four months, or a three-dose series (two, four, and six months). It is given orally, by putting drops in the baby’s mouth. The two vaccines have different dosing but similar efficacy and side effects, and your doctor is likely to use one or the other depending on their preferences.
- How well does the vaccine work? The vaccine is estimated to be 80% effective against rotavirus.
DTaP
- What is DTaP? The DTaP vaccine protects against three diseases: diphtheria, tetanus, and acellular pertussis (whooping cough).
- Diphtheria: A serious bacterial infection of the nose and throat. In the 1920s, this caused an estimated 13,000 to 15,000 deaths per year in the U.S. Currently it is extremely rare in the United States.
- Tetanus: Tetanus is caused by a toxin produced by a bacterial infection, typically after an injury. Prior to vaccination, there were an estimated 500 tetanus cases in the U.S. per year. The current number is less than 50.
- Pertussis: Otherwise known as whooping cough, this is a respiratory illness caused by bacteria. Prior to vaccination it caused several hundred thousand cases per year and an estimated 9,000 deaths in the U.S. Current case numbers are around 15,000 per year, with only 10 pertussis deaths per year in the U.S., mostly among young infants. However, pertussis rates have risen since a low in the early 1980s of under 5,000 a year.
- Vaccine basics: This vaccine is given at two months, four months, and six months. (There are also two boosters at 15 to 18 months and 4 to 6 years). Most women also get a related vaccine — Tdap — during pregnancy, which provides early protection to the infant. The Tdap vaccine protects against the same diseases, but because it’s a booster it has a lower dose of the pertussis vaccine.
- How well does the vaccine work? Both diphtheria and tetanus are effectively unknown outside of unvaccinated individuals; estimates suggest an efficacy close to 100% for both. For pertussis, efficacy is estimated at 98% for a year following the last dose in childhood, and 70% five years after that.
- Additional notes: This vaccine is typically given as a set covering all three diseases. There is a separate vaccine that covers only diphtheria and tetanus, but the pertussis vaccination only comes in the set.
Haemophilus influenzae type b (Hib)
- What is Hib? Hib is a bacterial infection that can cause serious complications, especially in babies and small children, including meningitis and pneumonia. Before widespread vaccination, it caused an estimated 20,000 serious cases in the U.S., and 1,000 deaths.
- Vaccine basics: Two doses at two months and four months, and a follow-up between a year and 15 months. (Sometimes a third dose is given at six months, depending on the timing of the first two.)
- How well does the vaccine work? The efficacy of these vaccines is about 95%. As a result of widespread vaccination, Hib cases are down over 99% relative to the period before vaccination.
Pneumococcal conjugate vaccine (PCV)
- What is pneumococcal disease? This is a name for any infection caused by pneumococcal bacteria, which can cause a wide range of infections throughout the body, including blood infections, brain infections, pneumonia, ear infections, and sinusitis. The vaccine protects against a variety of pneumococcal bacteria.
- Vaccine basics: This vaccine is given as a four-dose series — two, four, and six months, and then 12 to 15 months.
- How well does the vaccine work? The efficacy is 80%. Overall incidence of this disease in children has declined quickly since the vaccine has been introduced.
Polio vaccine
- What is polio? A viral disease that causes paralysis and weakness. Paralysis can persist and spread to the spinal cord and brain, making it difficult to breathe. Seen pictures of kids in an iron lung? These were used in the 1950s for children who were paralyzed temporarily due to poliovirus. Polio outbreaks before vaccination were large and deadly. A 1952 outbreak in the U.S. caused an estimated 60,000 cases, 3,000 deaths (across all ages), and 20,000 cases of paralysis.
- Vaccine basics: The polio vaccine was developed in 1955 and was widely viewed at the time as a miracle. It is given in four doses — two months, four months, sometime between six and 18 months, and at 4 to 6 years.
- How well does the vaccine work? Polio has been virtually eliminated in the United States. In 1979 the U.S. was declared polio-free. However, polio still circulates globally, which is why we still vaccinate children. Further, in 2022 an unvaccinated teenager in New York developed polio, which is a reminder that the virus is not gone.
- Additional notes: If you want to feel really good about vaccines and the miracles of science, I highly recommend the book Polio: An American Story.
MMR (measles, mumps, rubella) vaccine
- What is MMR? The MMR vaccine protects against three viruses.
- Measles is a viral illness that causes a rash and flu-like symptoms. Prior to widespread vaccination, there were an estimated 3 million to 4 million cases and 400 to 500 deaths from measles per year in the U.S. Measles is extremely contagious, and the virus can live on surfaces for a long period of time.
- Mumps is a contagious viral illness that causes jaw swelling, loss of appetite, and fatigue. Before vaccination, it caused about 160,000 illnesses per year in the U.S.
- Rubella: A viral illness that causes a rash, fever, and sore throat. Sometimes called “German measles.” Generally mild; currently very rare in the U.S.
- Vaccine basics: The MMR vaccine is typically given in a first dose between a year and 15 months, and a second dose at 4 years. If your child is at higher risk of measles exposure (for example, due to travel), doctors may do the first vaccine before age 1. However, children may in this case need three doses.
- How well does the vaccine work? Extremely well. Post-vaccination, both mumps and rubella are rarely seen in the U.S. In the case of measles, one dose of the vaccine provides an estimated 95% protection, and two doses provide an estimated 99%. This immunity seems to be durable through life and it is sterilizing, meaning that you cannot infect others with measles.
- Additional notes: Concerns are often raised about links between the MMR vaccine and autism. However, the data that underlies this idea was fabricated — literally, fabricated. The original paper on it was retracted, since the author had been dishonest about the selection of his sample of children and their symptoms. He was motivated, it seems, by a desire to have evidence to use in class-action lawsuits. In fact, there is a lot of excellent analysis showing no relationship between this vaccine and autism (here is just one example).
Varicella (aka chickenpox)
- What is chickenpox? If you are a child of the 1980s, as I am, you know. Viral illness. Itchy rash, fever, fatigue. Did I mention the itching? Before the vaccine, in the early 1990s, there were an estimated 4 million cases of chickenpox, over 10,000 hospitalizations, and 100 to 150 deaths per year. Generally, chickenpox is less serious when contracted in childhood, and having had it generates lifetime immunity. This is why my parents (like many others) had “chickenpox parties,” where they tried to purposely get us infected.
- Vaccine basics: One dose at 12 to 15 months, another at age 4 to 6. This is sometimes combined with the MMR vaccine and, whether combined or not, is generally given at the same time.
- How well does the vaccine work? With two doses, the protection is 92% against any disease and over 98% against severe disease. Chickenpox is now quite rare in the U.S., with an estimated 150,000 cases per year. Relative to having had chickenpox, those who are vaccinated are also less likely to develop shingles as an adult.
Hepatitis A
- What is hepatitis A? Hepatitis A is a contagious virus that causes liver disease. It’s spread through contaminated water and food, largely, or through poor personal hygiene. Before vaccination, children ages 2 to 18 had the highest rates of hepatitis. Prior to vaccination, the U.S. saw an estimated 270,000 infections annually. Though generally rare at this point, hepatitis A outbreaks became more common after 2016, relative to earlier years.
- Vaccine basics: Two-dose series, sometime between 12 and 24 months.
- How well does the vaccine work? Efficacy is thought to be close to 100% after two doses, with ongoing protection for as much as 20 years.
Vaccines 101
How do vaccines work?
When you get sick — with a virus or bacterial infection — your body makes antibodies to fight back. These are proteins that recognize, attach to, and kill whatever is causing the disease (the antigens). When you recover, your body retains these antibodies — and the memory of how to make them — so it can fight back more quickly if you are exposed to the same pathogen again. Vaccines work by exposing individuals to a virus or bacteria in a way that allows them to make antibodies against the virus or bacteria without making them sick.
Generally, this is done by exposing people to a killed form of the bacteria or virus or a live but weakened version. When delivered in this way, people do not get sick, but their body, recognizing an unfamiliar invader, creates antibodies to fight it. If you are then exposed to the real thing, the actual live pathogen, you have antibodies against it and will not get sick (or not as sick).
High levels of vaccination in a community overall can deliver herd immunity, where so many people are immune that the disease cannot get a foothold. This is important because it provides protection even for individuals who, for some reason, cannot get vaccinated themselves. This includes children who are too young for a vaccine, and those who have cancer or other immunocompromise.
Why do kids need multiple shots of the same vaccine?
For a number of vaccines, the schedule involves multiple shots. This is because having multiple exposures gives a stronger and longer-lasting level of protection. For pertussis, for example, there is a 55% reduction in hospitalization risk in the first year if your child gets one dose, but 83% for two or three doses.
Multiple shots of childhood vaccines happen for a different reason than seasonal vaccine boosters like flu or COVID. Those seasonal boosters are used because the viruses change over time. Childhood vaccine shots are the same across all doses; the goal is to enhance protection against a single pathogen.
What are general vaccine side effects?
Vaccines work by prompting an immune response in the body, which will commonly cause side effects like fatigue, fever, or crankiness. Many people find their child is in a bad mood after vaccines. This is an expected reaction to an immune challenge. It doesn’t mean the child has gotten sick from the vaccines.
There are some rarer side effects from vaccines. Children (or adults) can have allergic reactions. If the vaccine causes a fever, febrile seizures can happen (this is still rare but more likely with the MMR vaccine, in which it occurs in about 1 in 4,000 cases). And for children with immunocompromise, there are rare cases of more serious side effects from the measles vaccine.
Generally, kids can be given Tylenol or (if they are over six months) ibuprofen to address vaccine side effects. These treatments do slightly reduce the levels of antibody production, but not enough to matter for efficacy.
How do we know if vaccines are safe for children?
Vaccine safety is very heavily monitored by the government, in a system that is ingrained and will not change with a new administration. Before a vaccine is approved, safety trials are required. After approval, there is an adverse event reporting system, where doctors (or anyone else) can report adverse vaccine events. Many of these events are not actually due to the vaccines, but they are used to monitor. Because of this monitoring, even quite rare side effects can be identified.
This should give some broad safety reassurance. These vaccines have been given to millions and millions of children — in some cases hundreds of millions — which makes us confident that even rarer side effects would be seen if they were there.
Is there a reason to space vaccines out?
Typically, many vaccines are given at once, at regularly scheduled well-child visits. Some parents consider spacing out vaccinations so they are not all given at a single visit. Is there any reason to do this?
No. The immune system can respond to multiple challenges at once, so there is no reason to adapt the current vaccine schedule. Having said this: spaced-out vaccines are better than no vaccines, and if that makes you more comfortable with vaccinating, many doctors will be willing to do it. But it’s important to remember this agreement is generally not because they think it’s better to space them out than to do the normal vaccine schedule, but rather that some vaccines are better than none.
Why are some vaccines more effective than others?
There are some vaccines — the childhood measles vaccine is a classic example — that are incredibly effective. A child who is fully vaccinated for measles is not only extremely unlikely to get measles but is also extremely unlikely to spread measles. This is because the immunity delivered by the measles vaccine is extremely durable, and the vaccine generally delivers what is called sterilizing immunity. Basically, the length of time the pathogen takes to replicate is sufficiently long that the immune system response is faster, and it never really gets going. The transmission of measles is therefore cut off.
There are other vaccines, like the seasonal flu vaccine, where the effectiveness is lower. One reason for this is that there is some guesswork in making the flu vaccine, and depending on how close the match of the vaccine is to the circulating form of the virus, efficacy may be more or less. It’s nearly always the case that a flu vaccine lowers the risk of getting the flu and makes it less severe if you do get it, but it doesn’t always fully protect you.
A lot of these viruses are rare now — why are we still vaccinating against them?
It’s clear that vaccination has been an incredible public health victory. Diseases that killed millions of people, including children, are now rare. The flip side of that is that parents may wonder, what’s the point? No one gets diphtheria anymore, so why give your kid the vaccine?
The short answer is that it is only because of continued vaccination that these diseases are at bay. We have seen that pretty dramatically in the past several years, as measles vaccination rates have waned and measles outbreaks have occurred. The reality is that if we stopped vaccinating, a lot of these diseases would come back.
The bottom line
- The childhood vaccine schedule protects against diseases that collectively caused millions of illnesses and thousands of deaths annually before vaccination — diseases like measles, polio, and rotavirus.
- These vaccines are extremely effective (80-99% protection for most) and heavily monitored for safety through required trials and ongoing adverse event reporting that would detect even rare side effects across hundreds of millions of doses.
- There’s no evidence-based reason to space out vaccines — the immune system handles multiple challenges simultaneously, and the standard schedule is safe — though spaced-out vaccines are still better than none if that’s what makes you comfortable.
- Continued vaccination is the only reason these diseases remain rare; when vaccination rates drop, outbreaks return, as we’ve seen recently with measles.












Log in
Elephant in the room is covid vaccine at 6 months! Please address.
I’m surprised that you guys did not address the still-being-researched link between food allergies and infant vaccines. I do not want to spread misinformation, so I would love for ParentData to tackle this as an addendum. Not wading into the politics (spoiler: we are “pro vaccine” camp), our older daughter has a number of food allergies and had severe infant eczema, which often go together. Her first major flare ups of eczema happened after her 2 month and again her 4 month vaccine courses. And then of course we found out about her food allergies after we introduced solids later on (i.e. post 6 months). It has always been in the back of our heads as to whether there was a connection between the two. I’m not sure we would have done something differently, but we wish we had a clear picture of the science to inform the choices we made.
I wish your introductory messaging did not phrase the autism fear this way: “Add to that external conversations about possible links to autism or vaccine injury, and it’s not surprising that people have questions.” There are no possible links to autism. The misinformation campaign has been so disturbingly powerful, it’s so important key messaging be clear, concrete, and unequivocal. Public health messengers should not offer a “both sides” take on this one, as one side is simply false. Perhaps you could instead have written, “Add to that the misinformation campaign that has falsely linked vaccines to autism…”
My first test of anyone offering vaccine advice is whether they insist that the hepatitis b vaccine must be given at birth. Thanks for being honest!
I know this is a blog post and not a book, but the depth and rigor here leaves a lot to be desired…
Expecting Better was a hit because it didn’t just repeat public health guidelines (like this post does), but discussed the data and studies and methodologies that led to those guidelines. Then, the reader could judge for themselves which guidelines had legitimate backing and which were outdated rules of thumb or just generally unfounded.
There’s none of that here.
A lot of vaccine hesitancy feels legitimate because we don’t know anything about the research that led to, say, the Hep B vaccine being given at birth. What studies showed it’s safe? What was their methodology, how long did they follow the children, etc. The aluminum content of the vaccines (compounding when many are given at once) is a common concern, and that wasn’t even mentioned here. Finally, there are studies that show harm. Are these bad studies? What was their methodological error?
Each vaccine should be a cost/benefit decision, and this post gives no useful information about the costs and benefits…
I say this as someone who was eagerly awaiting Emily’s vaccine post. Color me disappointed.
Agreed.
I actually think this critique could be said about most of the recent newsletters. To be honest, feels like Emily is no longer the one writing them.
Yea, this reads like a chatgpt output of “give me 3 bullet points for each childhood vaccine.”
Agreed!!
If you could say any more about RSV shots for kids for whom mom had one pre natally thatbwould be helpful. My daughter was born in March; on our parents’ list for kids born that month, a few of us (who got the shot when pregnant) were able to get our kids vaccinated the following winter but many people were told they couldn’t, primarily due to insurance reasons. But it seems for a March baby another shot in the fall would be beneficial since it has been over 6 months.
Thank you for this, Emily! Vaccines are such an important and effective public health measure for the population!
A few points:
HPV is now given at age 9. While many parents would like to delay this vaccine, it is most effective if given at age 9. If the series is started before age 15, there are only two shots in the series, but if the series is started after age 15, three shots are required in the series to reach effectiveness.
The Hepatitis B virus can live for a long time in dried blood and body fluids. That is why it is important to get this vaccine in infancy even though the virus follows the pathway of blood and body fluid exposure.
HiB vaccine protects against the severe symptom of epiglottitis, a symptom which is immediately life threatening. This vaccine is extremely effective with this protection.
Rubella, which causes only mild symptoms in a child, can be devastating to a fetus, causing intellectual impairment and/or deafness in many cases. Protecting children with MMR protects pregnant women from contracting rubella and thereby protects fetuses.
Some brands of vaccines, particularly for rotavirus and HiB, have different dosing schedules. If your provider tells you that your child needs an additional dose of HiB at 6 months, or does not need a third dose of Rotavirus, it is because of the brand of vaccine. There are also different combinations of vaccines which can reduce the number of jabs.
The schedule that you shared applies to the U.S.: other countries have other schedules. For example, many countries give a form of a meningococcal vaccine in infancy, while in the U.S. we wait until age 11 for this. This may be subject to change if surveillance shows different patterns of incidence.
Many of these vaccines can be given earlier than what is shown on this schedule. The two month vaccines can be given at 6 weeks. MMR can be given at 6 months but then needs to be repeated at 12 months. This is sometimes done when there are outbreaks, and you can request this if your baby is in an area with an outbreak or will be going into such an area.
would love if you addressed the “heavy metals” – especially aluminum that is used in the vaccines and any causations. Thank you!!!
Yes I came here to ask about this. I have a mentor that’s adamantly anti vax now after having a chronic cough diagnosed as a vaccine injury from H1N1 vax during her pregnancy. The cough has persisted for 15 years now. She has since “researched extensively” & says the buildup of the metals / preservatives in the vaccines are incredibly inflammatory in the body & have all sorts of negative consequences…that some vaccines are necessary, but most are for profit for big pharma to ensure we stay sick & therefore profitable……..would love these common talking points addressed to have better responses prepared! Thank you!!
You may find this website helpful, from the Children’s Hospital of Philadelphia: https://www.chop.edu/vaccine-education-center/vaccine-safety/vaccine-ingredients
For example, on the page about Aluminum in vaccines, it reads: “The aluminum contained in vaccines is similar to that found in a liter (about 1 quart or 32 fluid ounces) of infant formula. While infants receive about 4.4 milligrams* of aluminum in the first six months of life from vaccines, they receive more than that in their diet. Breast-fed infants ingest about 7 milligrams, formula-fed infants ingest about 38 milligrams, and infants who are fed soy formula ingest almost 117 milligrams of aluminum during the first six months of life.”
You may find this website helpful, from the Children’s Hospital of Philadelphia: https://www.chop.edu/vaccine-education-center/vaccine-safety/vaccine-ingredients
For example, on the page about Aluminum in vaccines, it reads: “The aluminum contained in vaccines is similar to that found in a liter (about 1 quart or 32 fluid ounces) of infant formula. While infants receive about 4.4 milligrams* of aluminum in the first six months of life from vaccines, they receive more than that in their diet. Breast-fed infants ingest about 7 milligrams, formula-fed infants ingest about 38 milligrams, and infants who are fed soy formula ingest almost 117 milligrams of aluminum during the first six months of life.”