






As we get older, that means, among other things, cancer screening. The landscape of cancer screening can seem complicated: when to start, which tests to use, whether some are better than others. I’ve written before about mammograms, and today we’ll move to the colon. I’ll start with background on changes in colon cancer over time — especially given some scary headlines about cancer in younger people — and then talk through screening options.
A quick note: I will use “colon cancer” here to refer to “colorectal cancer” since it is the terminology most people are familiar with. But this type of cancer appears in both the colon and the rectum.

Is colon cancer increasing among younger people?
As mentioned above, we’ve seen an uptick in news lately about the increase in colon cancer among younger people. This trend is present, but it is useful to put it in context.
Overall, colon cancer cases have declined over time, with a decrease of about 33% since 1999. The estimated rate in 2022 was 35.1 per 100,000 people. Probably the most important element of colon cancer risk is age. The graph below, from this summary paper, shows the incidence of colon cancer by age group in 2020. Older people are orders of magnitude more likely to be diagnosed than younger people.
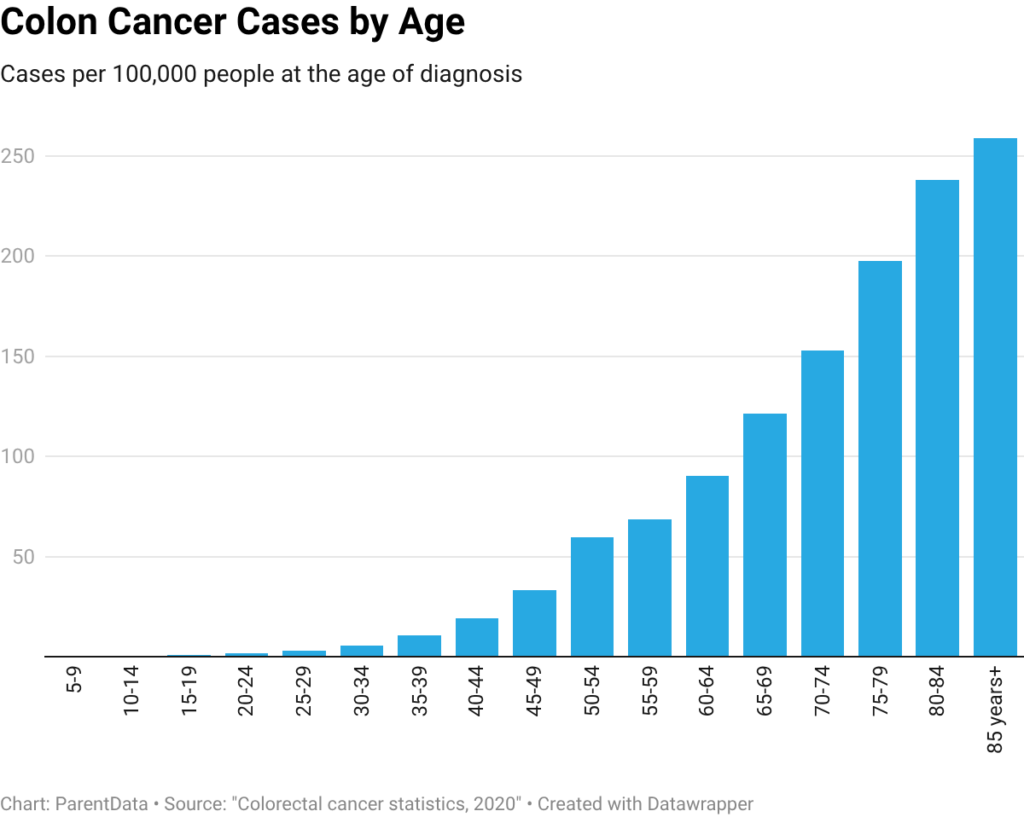
Colon cancer cases in older people have declined over time, probably due to better detection of early precancerous lesions and reductions in smoking. Because this older group is so much more likely to be diagnosed overall, a reduction in risk in that group translates to a reduction in risk overall. However, this overall reduction masks an increase in cases in people under 50, especially men.
This excellent paper on early-onset cancer cases over time shows an increase in colon cancer cases among people under 50 of 2.2 cases in 100,000 for men and 1.1 in 100,000 for women. Put in the context of the graph above, as a share of the cases in this group, this number seems moderately large. But it still leaves these younger age groups far less likely to be diagnosed than older age groups. (This paper also looks at other types of cancer in younger people, and I talked more about breast cancer rates in this article.)
In all, there does seem to be a statistically significant increase in colon cancer in younger people, but the overall risk is still very small, and age remains by far the most significant risk factor. In terms of why we are seeing this increase, it’s not clear. But there are a number of risk factors for colon cancer — obesity, lack of fiber, a high-fat diet — that have increased over time and may play a role. A 2023 finding that the use of GLP-1s lowers the risk of colon cancer does suggest that something about food and metabolism matters here.
When should you start screening for colon cancer?
Although the recent discussions have largely focused on colon cancer in younger people, screening for colon cancer generally does not start until age 45. A reasonable question to ask first is why we do not screen everyone, if these rates are going up. The answer is that because these cancers are still so rare in these younger age groups, it doesn’t make sense to screen. It’s both that it doesn’t make sense financially and also that it probably doesn’t make sense from an individual standpoint. The idea of colon cancer is frightening, but the risk is so small that the time, cost, and discomfort of screening — along with the emotional cost of false positives — make it a bad idea for most people. However, if you have a medical condition like Lynch syndrome or inflammatory bowel disease, or any potentially concerning symptoms (unexplained weight loss, blood in stool), please see a doctor, regardless of age.
Once you age up to and past 45, colon cancer screening is recommended. The U.S. Preventive Services Task Force strongly recommends screening from ages 50 to 75 and also suggests screening between 45 and 50. Its assessment of the value in this earlier age group is lower because the risk in that group is lower.
If you have risk factors — a family history or any personal history — screening is recommended earlier (perhaps age 40), and there may be more push to screen with colonoscopy rather than other options (more on that below). Family history is really important here — because family history matters a lot in screening and in risk, please talk to your parents (if you can!) about their own colonoscopies and any other family history. It’s a great topic to bring up at a holiday meal to move people away from politics!
The goal of colon cancer screening is to detect cancer, or precancerous growths, when they are still treatable. The most important determinant of survival in colon cancer is the stage at which it is detected. Early-stage colon cancers can typically be treated and, in many cases, cured with surgery to remove them. Chemotherapy and radiation are sometimes, but not always, needed. The earlier the detection, the better the prognosis.
Screening for colon cancer reduces mortality — I’ll get into this in more detail below, but adherence to routine screening in the recommended way may reduce colon cancer deaths by an estimated 20 to 25 per 1,000 over a lifetime.
This suggests that some type of colon cancer screening is a good idea. The question is, which one?
What are the types of screening options?
Broadly, there are two approaches to screening for colon cancer. One — the most traditional — is a colonoscopy (or a sigmoidoscopy). In this procedure, a flexible tube is inserted in the rectum and snaked around the colon. A camera is used to visualize what is going on and observe any lesions. During a colonoscopy, “polyps” or precancerous growths can be removed, which prevents cancer from occurring.
A second approach is to test your poop directly, using either a fecal immunochemical test (FIT) or a FIT plus DNA testing (there are a couple of other options in this space as well, but these are the most common). The second of these, the FIT-DNA test, is marketed in the U.S. as Cologuard.
Both of these tests involve collecting poop, usually at home, and shipping it off to a lab where it is tested for signs of cancer. This includes testing for signs of blood that might be shed by lesions in the colon and, in the FIT-DNA test, looking for signs of cancer DNA. In these tests, if the test is positive (if it suggests there could be a risk of cancer), a colonoscopy would be used as follow-up.
The graph below, which was helpfully compiled by UpToDate from several sources, shows the efficacy of these three options in terms of the detection of both smaller precancerous lesions (called adenomas) and the detection of colon cancer.
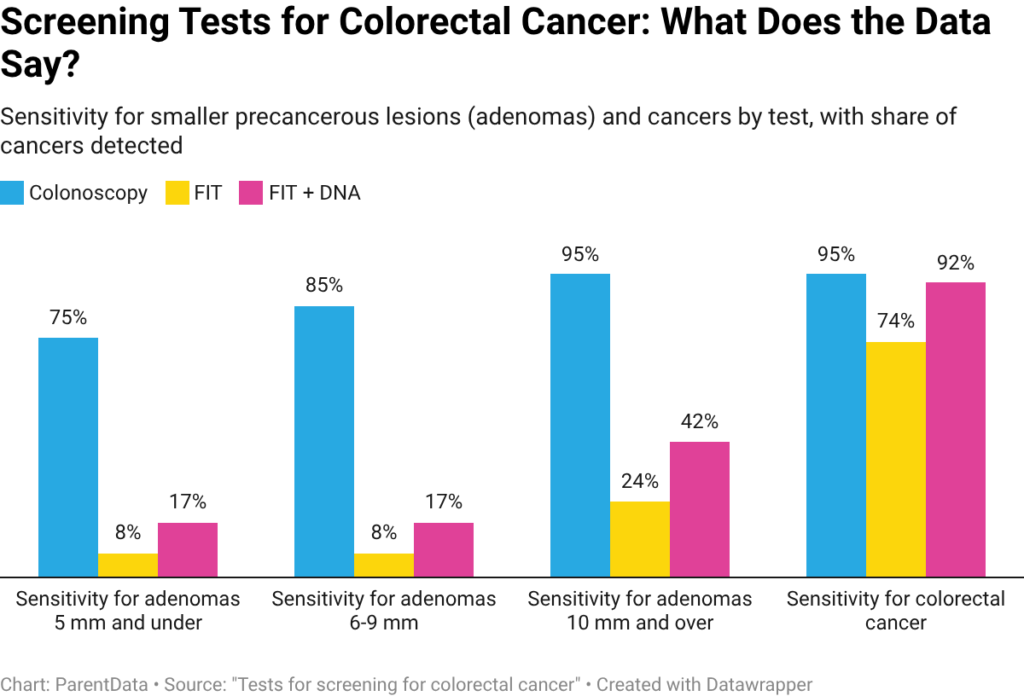
There are a couple of things to note from this graph. First, the colonoscopy is the gold standard. It does the best job of detecting both colon cancer overall and smaller adenomas. The FIT-DNA is effectively as good as the colonoscopy for finding colon cancer. However, while both of the poop collection options do quite well for colon cancer detection, they are more likely to miss smaller adenomas, especially the FIT alone. A colonoscopy can also find smaller polyps, which can be removed and prevent further development.
When we look at the number of deaths averted, though, these tests all perform similarly in preventing deaths. This is likely because these poop-based technologies detect early enough to lower mortality, even if it might be on average later than a colonoscopy. In addition, because the poop-based technologies are used more frequently (typically, yearly rather than every 5 or 10 years), they get more bites at the apple, so to speak.
This data alone suggests that there are multiple good screening options. Which one you want to choose depends on a number of factors, including:
- Your underlying risk: For people with a family or personal history of cancer or polyps, going straight for a colonoscopy may be a better option.
- Your age: For older people without a history of colon issues, the noninvasive option may be completely fine because colon cancer spreads slowly, and detection in (say) an 80-year-old has different implications.
- Insurance and cost: A colonoscopy will generally be covered by your insurance. Cologuard may also be covered. However, if you screen positive on a Cologuard, you may need a diagnostic colonoscopy, which may not be covered by insurance. This is worth asking your doctor about before you choose.
- Overall preference: A lot of people are scared of a colonoscopy (you shouldn’t be — I try to alleviate those fears below). But if the colonoscopy feels too daunting, it would be much better to do something than nothing. Pooping in a box is a great option if the full procedure doesn’t sound like something you can commit to.
What is a colonoscopy like?
If you’ve never had one, a colonoscopy can seem daunting and scary. I am with you on this — I was scared before I got mine, too! But the reality is far less bad than you think. Here’s the rundown of what you can expect.
For 24 hours before your procedure (try to schedule in the morning), you eat a mostly liquid diet. This can include broth and jello, and I promise it is not as bad as you think it will be — just get some protein-heavy broth packets, and you’ll be fine.
Beginning the afternoon before, you then drink (in two doses) a foul-tasting beverage. For me, this was the worst part of the whole thing. You then poop a lot. I was concerned this would be like having a terrible bout of the norovirus, but it was not. It was just a lot of poop. My recommendation: hole yourself up away from your family, put on a Netflix show to binge, tell work you are unavailable, and try to treat this like a vacation with a lot of bathroom breaks.
The next day, you go in for the colonoscopy. It’s easy! They put you to sleep, do the procedure, and wake you up to tell you how it went, and then you go home to rest for the rest of the day (and refuel).
I will tell you with complete honesty: this was not nearly as bad as I feared.
Closing thoughts
I want to acknowledge that cancer screening may freak you out. By getting screened, we are acknowledging that the result could be bad. It can often feel easier to just pretend everything is definitely fine and not get screened. When we choose to get tested, we force ourselves to have some anticipatory experience of the bad outcome, which is unpleasant.
Please keep in mind here that there is a reason for this screening — and it’s a good one. If you detect colon cancer early, it is extremely treatable. So if you’re over 45 and you haven’t done this yet, now is the time! Pick your approach and get it done. You’ll be glad you did.
The bottom line
- Colon cancer has been decreasing over time overall, but increasing among younger people (although it is still very rare in people under 50).
- Colon cancer screening is recommended for people 45 and up, and especially for those above 50. If you have risk factors, you may start screening earlier (usually around age 40).
- The colonoscopy is the gold standard, but fecal testing has similar survival benefits and can be done from your own home.
- Get screened! Seriously! Just do it. It is not as scary as you think it will be.













Log in
I did the fecal test that you mail in, and they told me it would be 3 years before I’d need to do it again.
I’m wondering how the fecal tests compare to colonoscopies on illness/quality of life, not just mortality. Also I’d factor in the (small but real) colonoscopy complication rate. For someone at average risk, do colonoscopies make sense as opposed to a stool test?
Also factor in that a second person typically is needed to take time off work to drive the patient home, unless the patient can walk home or something. They legally can’t allow you to take a taxi.
Agreed with each of your good Qs and points. Hope Emily addresses them. Just went thru this process with my wife. Living in a rural area, colonoscopy was 1 day off work for each of us, then 1/2 day for her to “hear” the results in person. Driving rural roads. Hence the appeal of home tests to me.